Uterus is a vital reproductive organ and is associated with various benign and malignant pathologies. Surgical removal of uterus is known as hysterectomy. It can be performed either through abdominal or vaginal route or with the help of minimal invasive surgical procedures like laparoscope. There is diagnostic and therapeutic significance of performing histopathological examinations of hysterectomy specimens or any surgically excised specimens. The aim of the study was to evaluate clinical indications for hysterectomy and the histopathological features of varied lesions of uterus and cervix and their distribution in relation to age at a tertiary care hospital. This is a retrospective observational study conducted in Department of Obstetrics & Gynecology, Rama Medical College, Hospital & Research Center from July 2019 to March 2020. A total 250 patients were included in the study with age range from 19-70 years. Histopathological examination reports were analyzed and compared with clinical diagnosis. Histopathological examination of all the surgically excised specimens should be done regardless of its benign indication as this helps to correlate with the pre-operative clinical diagnosis and provides the final diagnosis.
Keywords
Hysterectomy
Histopathological Examination
Endometrial Changes
Myometrial Changes
Cervical Changes
INTRODUCTION
The female genital tract consists of the uterine corpus and cervix and the uterine corpus consists of endometrium and myometrium[1]. Uterus is a vital reproductive organ and is associated with various benign and malignant pathologies [2]. Surgical removal of uterus is known as hysterectomy and is the most commonly performed major surgery in all gynecological settings. It is the definitive treatment for various benign and malignant conditions of female reproductive tract e.g., fibroid, adenomyosis, dysfunctional uterine bleedings, uterine prolapse, post-partum hemorrhage and malignant lesions of uterus, ovaries and cervix [3]. Charles Clay was the first to perform total hysterectomy in 1929 in England [4]. It is the second most commonly performed surgery after cesarean section in obstetrics and gynecological settings [5]. It can be performed either through abdominal or vaginal route or with the help of minimal invasive surgical procedures like laparoscope. There is diagnostic and therapeutic significance of performing histopathological examinations of hysterectomy specimens or any surgically excised specimens [6]. Hence, this study was conducted to study the clinical and histopathological patterns of changes in the uterus and cervix of the hysterectomy specimens. The aim of the study was to evaluate clinical indications for hysterectomy and the histopathological features of varied lesions of uterus and cervix and their distribution in relation to age at a tertiary care hospital.
Although hysterectomy is ultimate treatment of many pathologies but advancement in imaging technique for diagnosis and advent of novel treatment like endometrial ablation, uterine artery embolization, hysteroscopic myomectomy, MRI focused ultrasound fibroid ablation, radiofrequency ablation and hormonal IUD (mirena), many hysterectomies can be prevented.
MATERIALS AND METHODS
This is a retrospective observational study conducted in Department of Obstetrics & Gynecology, Rama Medical College, Hospital & Research Center from July 2019 to March 2020. A total 250 patients were included in the study with age range from 21-70 years. All the procedures of hysterectomy done for benign indications in the department during this study period were included. Clinical data was collected about age, reproductive status, history, indication for hysterectomy; type of surgical intervention was recorded from patient’s record file. Histopathological examination reports were analyzed and compared with clinical diagnosis.
The specimens were grossed by the pathologists. All the specimens were fixed in 10% formalin and tissue sections were taken for processing and paraffin block preparation. The paraffin blocks were sectioned and stained by H & E stain. Microscopical examination was performed for histopathological diagnosis.
RESULTS
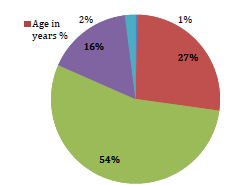
The study included 250 patients who underwent hysterectomy during the study period. According to Table 1, the number of patients who underwent hysterectomy was maximum in the age group of 41-50 years (54.4%), followed by 31-40 years (26.8%), 51-60 years (16.4%), >60 years (2%) and the least were <30 years (0.4%). That is also shown in a pie chart in figure 1.
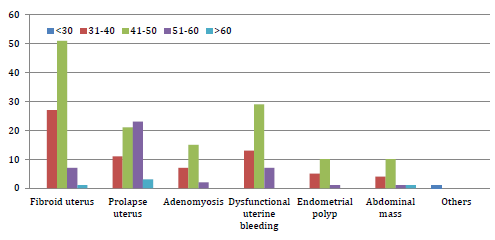
The most common indication for hysterectomy was fibroid uterus (34.4%), followed by prolapse uterus (23.2%), dysfunctional uterine bleeding (19.6%), adenomyosis (9.6%), endometrial polyp (6.4%), abdominal mass (6.4%) and others (0.4%). The indication for the only hysterectomy done in age group <30 years was obstetric hysterectomy due postpartum hemorrhage with placenta accreta. The most common indications in other age groups were fibroid uterus in 31-40 years (40.29%) and in 41-50 years (37.5%), while prolapse uterus in 51-60 years (56.09%) and in age >60 years (60%).
Figure 1: Age distribution of patients
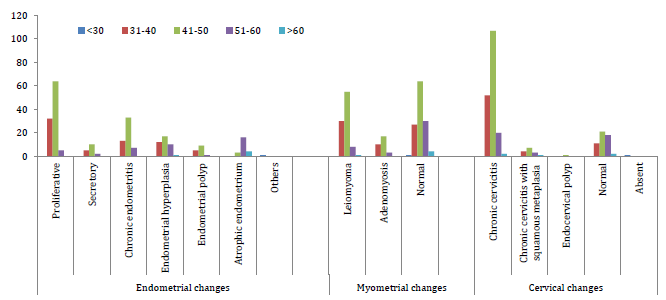
The most common histopathological finding in the endometrium was proliferative endometrium (40.4%), followed by chronic endometritis (21.2%), endometrial hyperplasia (16%), endometrial polyp (6%), atrophic endometrium (9.2%), secretory endometrium (6.8%) and others (0.4%). The most common histopathological finding in the endometrium of the in-age group <30 years was decidual changes and chorionic villi implanted on the surface of myometrium with no intervening decidua. The most common histopathological finding in the endometrium in other age groups was proliferative endometrium in 31-40 years (47.76%) and in 41-50 years (47.05%) while atrophic endometrium in 51-60 years (39.02%) and in age >60 years (80%).
The most common histopathological finding in the myometrium was normal myometrium (50.4%), followed by leiomyoma (37.6%) and adenomyosis (12%). The most common histopathological finding in the myometrium was normal myometrium in age groups 41-50 years (47.05%), 51-60 years (73.17%) and in age >60 years (80%) while the most common histopathological finding in the myometrium was leiomyoma in age group of 31-40 years (44.78%).
Table 1: Age distribution of patients.
Age in years
No. of patients
%
< 30
1
0.4
31-40
67
26.8
41-50
136
54.4
51-60
41
16.4
> 60
5
2
Table 2: Indications for hysterectomy.
Indication
Age in Years
< 30
31 - 40
41 - 50
51 - 60
> 60
Total
Fibroid uterus
0
27
51
7
1
86
Prolapse uterus
0
11
21
23
3
58
Adenomyosis
0
7
15
2
0
24
Dysfunctional uterine bleeding
0
13
29
7
0
49
Endometrial polyp
0
6
20
2
0
16
Abdominal mass
0
4
10
1
1
16
Others
1
0
0
0
0
1
Figure 2: Indications for hysterectomy
Table 3: Histopathological Findings
Histopathological Findings
Age in Years
< 30
31 - 40
41 - 50
51 - 60
> 60
Total
Endometrial changes
Proliferative
0
32
64
5
0
101
Secretory
0
5
10
2
0
17
Chronic endometritis
0
13
33
7
0
53
Endometrial hyperplasia
0
12
17
10
1
40
Endometrial polyp
0
5
9
1
0
15
Atrophic endometrium
0
0
3
16
4
23
Others
1
0
0
0
0
1
Myometrial changes
Leiomyoma
0
30
55
8
1
94
Adenomyosis
0
10
17
3
0
30
Normal
1
27
64
30
4
126
Cervical changes
Chronic cervicitis
0
52
107
20
2
181
Chronic cervicitis with squamous metaplasia
0
4
7
3
1
15
Endocervical polyp
0
0
1
0
0
1
Normal
0
11
21
18
2
52
Absent
1
0
0
0
1
Figure 3: Histopathological Findings
The most common histopathological finding in the cervix was chronic endocervicitis (72.4%), followed by chronic cervicitis with squamous metaplasia (6%), endocervical polyp (0.4%) and normal cervix (20.8%). The cervix was absent in age group <30 years as it was a supracervical hysterectomy. The most common histopathological finding in the cervix was chronic endocervicitis in age groups 31-40 years (77.6%), 41-50 years (78.6%), 51-60 years (48.78%) and >60(40%).
DISCUSSION
Hysterectomy is the most commonly performed gynecological procedure worldwide and its number may vary according to region, community and social factors.
The most common age group undergoing hysterectomy was 41-50 years with the mean age of 44.28 yrs. The results are similar to Siwatch S et al. [7], Zaid et al. [8] and Sreedhar V et al. [9].
In our study, the most common indication for hysterectomy was fibroid uterus, which is similar to the study done by Verma D10 et al and Jandial R [11] et al. In a study conducted by Siwatch S et al. [7]most common indication for age group<30 years was postpartum hemorrhage, 30-45 years was fibroid, 45-60 years was fibroid and >60 years was prolapsing uterus. All these results are similar to our study. On histopathological examination, most common endometrial finding was proliferative endometrium. This result is similar to study done by Jindal R et al. [11] and Verma D et al. [10]. The most common myometrial finding was leiomyoma. This result was similar to study by Jindal R et al. [11] and Sreedhar V et al. [9]. The most common histopathological finding in cervix was chronic cervicitis, similar findings were observed by Jindal R et al. [11] and Zaid et al. [8].
CONCLUSION
Hysterectomy is the most commonly performed surgery for gynecological indications. Histopathological examination of all the surgically excised specimens should be done regardless of its benign indication as this helps to correlate with the pre-operative clinical diagnosis and provides the final diagnosis.
REFERENCE
Qamar-ur-Nisa. "Hysterectomies, an audit at a tertiary care hospital." Professional Med J, vol. 18, no. 1, 2011, pp. 45-50.
Kjerulff, Kristen H. "Chronic gynecological conditions reported by US women: findings from the National Health Interview Survey, 1984 to 1992." American Journal of Public Health, vol. 86, no. 2, 1996, pp. 195-199.
Nausheen, Fariha. "Hysterectomy: the patient's perspective." Annals of King Edward Medical University, vol. 10, no. 4, May 2016, pp. 339-341.
Gupta, Geeta. "Hysterectomy: a clinico-pathological correlation of 500 cases." Internet Journal of Gynecology and Obstetrics, vol. 14, no. 1, 2010.
Wu, Jennifer M. "Hysterectomy rates in the United States, 2003." Obstetrics & Gynecology, vol. 110, no. 5, 2007, pp. 1091–1095.
Silverberg, Stanley G., et al.Silverberg’s Principles and Practice of Surgical Pathology and Cytopathology. 4th ed., vol. 2, Elsevier, 2006, p. 1935.
Siwatch, Sujata. "Histopathological audit of hysterectomy specimens in a tertiary care hospital." Sri Lanka Journal of Obstetrics and Gynecology, vol. 3, 2007, pp. 155-158.
Mohamed, Suad O. "Histopathological findings in hysterectomy specimens: A retrospective study." Middle East Journal of Internal Medicine, vol. 10, no. 1, 2017, pp. 17-22.
Sreedhar, Vijay V. "Histopathological spectrum of lesions of hysterectomy specimens: a study of 200 cases." Saudi Journal of Pathology and Microbiology, vol. 1, no. 2, Jul.-Sept. 2016, pp. 54-59.
Verma, Deepti. "Analysis of histopathological examination of the hysterectomy specimens in a north Indian teaching institute." International Journal of Research in Medical Sciences, vol. 4, no. 11, Nov. 2016, pp. 4753-4758.
Jandial, Ruchika. "Histopathological analysis of hysterectomy specimens in a tertiary care centre: study of 160 cases." International Surgery Journal, vol. 6, 2019, pp. 2856-2859.
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Applied Medical Sciences and Research open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Advertisement
Recommended Articles
Research Article
Systemic Inflammatory Markers in Patients with Combined Otitis Media and Rhinosinusitis
Mohammed Qasim Mohammed,
...
Abdulkareem Hussien Dabi
Published: 28/01/2026
Download PDF
Cite
x
APA
Qasim Mohammed, M., A. Mohammed Ali, W. & Hussien Dabi, A. (2026). Systemic Inflammatory Markers in Patients with Combined Otitis Media and Rhinosinusitis. Himalayan Journal of Applied Medical Sciences and Research, 7(1), 1-5.
MLA
Qasim Mohammed, Mohammed, Watheq A. Mohammed Ali and Abdulkareem Hussien Dabi. "Systemic Inflammatory Markers in Patients with Combined Otitis Media and Rhinosinusitis." Himalayan Journal of Applied Medical Sciences and Research 7.1 (2026): 1-5.
Chicago
Qasim Mohammed, Mohammed, Watheq A. Mohammed Ali and Abdulkareem Hussien Dabi. "Systemic Inflammatory Markers in Patients with Combined Otitis Media and Rhinosinusitis." Himalayan Journal of Applied Medical Sciences and Research 7, no. 1 (2026): 1-5.
Harvard
Qasim Mohammed, M., A. Mohammed Ali, W. and Hussien Dabi, A. (2026) 'Systemic Inflammatory Markers in Patients with Combined Otitis Media and Rhinosinusitis' Himalayan Journal of Applied Medical Sciences and Research 7(1), pp. 1-5.
Vancouver
Qasim Mohammed M, A. Mohammed Ali W, Hussien Dabi A. Systemic Inflammatory Markers in Patients with Combined Otitis Media and Rhinosinusitis. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Association Between Oxidative Stress Biomarkers and Age-Related Hearing Loss: A Hospital-Based Case–Control Study
Watheq A. Mohammed Ali,
...
Mohammed Qasim Mohammed
Published: 24/01/2026
Download PDF
Cite
x
APA
Mohammed Ali, W. A., Hussien Dabi, A. & Qasim Mohammed, M. (2026). Association Between Oxidative Stress Biomarkers and Age-Related Hearing Loss: A Hospital-Based Case–Control Study. Himalayan Journal of Applied Medical Sciences and Research, 7(1), 1-5.
MLA
Mohammed Ali, Watheq A., Abdulkareem Hussien Dabi and Mohammed Qasim Mohammed. "Association Between Oxidative Stress Biomarkers and Age-Related Hearing Loss: A Hospital-Based Case–Control Study." Himalayan Journal of Applied Medical Sciences and Research 7.1 (2026): 1-5.
Chicago
Mohammed Ali, Watheq A., Abdulkareem Hussien Dabi and Mohammed Qasim Mohammed. "Association Between Oxidative Stress Biomarkers and Age-Related Hearing Loss: A Hospital-Based Case–Control Study." Himalayan Journal of Applied Medical Sciences and Research 7, no. 1 (2026): 1-5.
Harvard
Mohammed Ali, W. A., Hussien Dabi, A. and Qasim Mohammed, M. (2026) 'Association Between Oxidative Stress Biomarkers and Age-Related Hearing Loss: A Hospital-Based Case–Control Study' Himalayan Journal of Applied Medical Sciences and Research 7(1), pp. 1-5.
Vancouver
Mohammed Ali WA, Hussien Dabi A, Qasim Mohammed M. Association Between Oxidative Stress Biomarkers and Age-Related Hearing Loss: A Hospital-Based Case–Control Study. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Clinical and Functional Outcomes of Interlocking and Küntscher Nailing in the Management of Femoral Shaft Fractures: A Prospective Study
Ahmed Abdalzahra Mohaisen ,
...
Mohammed Saad Abdulzahra
Published: 10/01/2026
Download PDF
Cite
x
APA
None, A. A. M., None, H. A. A. & None, M. S. A. (2026). Clinical and Functional Outcomes of Interlocking and Küntscher Nailing in the Management of Femoral Shaft Fractures: A Prospective Study. Himalayan Journal of Applied Medical Sciences and Research, 7(1), 1-7.
MLA
None, Ahmed Abdalzahra Mohaisen, Hassan Ali Abid and Mohammed Saad Abdulzahra . "Clinical and Functional Outcomes of Interlocking and Küntscher Nailing in the Management of Femoral Shaft Fractures: A Prospective Study." Himalayan Journal of Applied Medical Sciences and Research 7.1 (2026): 1-7.
Chicago
None, Ahmed Abdalzahra Mohaisen, Hassan Ali Abid and Mohammed Saad Abdulzahra . "Clinical and Functional Outcomes of Interlocking and Küntscher Nailing in the Management of Femoral Shaft Fractures: A Prospective Study." Himalayan Journal of Applied Medical Sciences and Research 7, no. 1 (2026): 1-7.
Harvard
None, A. A. M., None, H. A. A. and None, M. S. A. (2026) 'Clinical and Functional Outcomes of Interlocking and Küntscher Nailing in the Management of Femoral Shaft Fractures: A Prospective Study' Himalayan Journal of Applied Medical Sciences and Research 7(1), pp. 1-7.
Vancouver
Ahmed Abdalzahra Mohaisen AAM, Hassan Ali Abid HAA, Mohammed Saad Abdulzahra MSA. Clinical and Functional Outcomes of Interlocking and Küntscher Nailing in the Management of Femoral Shaft Fractures: A Prospective Study. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jan;7(1):1-7.
Download PDF
Research Article
Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community
Vishal Dhatwalia,
Swati Chandel
Published: 10/12/2024
Download PDF
Cite
x
APA
Dhatwalia, V. & Chandel, S. (2024). Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research, 5(2), 1-5.
MLA
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5.2 (2024): 1-5.
Chicago
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5, no. 2 (2024): 1-5.
Harvard
Dhatwalia, V. and Chandel, S. (2024) 'Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community' Himalayan Journal of Applied Medical Sciences and Research 5(2), pp. 1-5.
Vancouver
Dhatwalia V, Chandel S. Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research. 2024 Jul;5(2):1-5.
Mishra, S., Garg, P. & Divedi, P. (2021). Retrospective Analysis of Histopathological Examination of Hysterectomy Specimens in A Tertiary Care Centre. Himalayan Journal of Applied Medical Sciences and Research, 2(2), 1-4.
MLA
Mishra, Shweta, Paridhi Garg and Pragati Divedi. "Retrospective Analysis of Histopathological Examination of Hysterectomy Specimens in A Tertiary Care Centre." Himalayan Journal of Applied Medical Sciences and Research 2.2 (2021): 1-4.
Chicago
Mishra, Shweta, Paridhi Garg and Pragati Divedi. "Retrospective Analysis of Histopathological Examination of Hysterectomy Specimens in A Tertiary Care Centre." Himalayan Journal of Applied Medical Sciences and Research 2, no. 2 (2021): 1-4.
Harvard
Mishra, S., Garg, P. and Divedi, P. (2021) 'Retrospective Analysis of Histopathological Examination of Hysterectomy Specimens in A Tertiary Care Centre' Himalayan Journal of Applied Medical Sciences and Research 2(2), pp. 1-4.
Vancouver
Mishra S, Garg P, Divedi P. Retrospective Analysis of Histopathological Examination of Hysterectomy Specimens in A Tertiary Care Centre. Himalayan Journal of Applied Medical Sciences and Research. 2021 Jul;2(2):1-4.