Background: Ophthalmic manifestations of HIV infection are diverse. Both anterior and posterior segments of the eye can be involved and it may even lead to blindness.Keratoconjunctivitis sicca or dry eye occurs in later stages of the disease in 10 -20% of the patients. Aim: Present study was planned to see the correlation between level of CD4 count with the severity of dry eye in HIV seropositive patients. Material and Methods: The study was a hospital based cross – sectional study where 120 HIV-positive patients between 18 to 50 year of age group, registered at the ART centre and referred to Ophthalmology OPD for ocular complaints were included in the study. Subjects were investigated for dry eye with ocular surface disease index score (OSDI), Rose Bengal staining, Schirmers test 1 with and without anaesthesia and Tear Film Break Up Time (TBUT). Results: Significant mild positive correlation was seen between CD4 count and Schirmer-1 test without anaesthesia score (r value = 0.23; p value<0.001), Schirmer -1 with anaesthesia score (r value = 0.22; p value<0.001), Tear Film Breakup Time (TBUT) (r value =0.28; p value <0.01) but no correlation was seen with OSDI score (r value = -0.01; p value =0.83). Conclusion: Dry eye in people with HIV should not be looked down upon and should be treated for the same. CD4 count can also give indication severity of dry eye.
Keywords
Tear Film Break Up Time
Dry eye
CD4 Count
Schirmer-1 Test
INTRODUCTION
HIV (Human Immunodeficiency Virus) continues to be a major global public health issue, having claimed more than 39 million lives so far [1]. Acquired Immunodeficiency syndrome (AIDS) is one of the most feared infectious disease of the late 20th century. Since its discovery in 1981, AIDS has emerged as a global health problem. Thirty years after its discovery, virus has reached virtually every corner of the globe [2]. India has a large number of patients with AIDS, which is the third largest population of this group in the world [3].
According to a report which was made by the National AIDS Control Organization, 2017-2018, adult HIV prevalence in India was estimated at 0.26% (0.22% – 0.32%). The total number of people living with HIV (PLHIV) in India is estimated to be around 21.40 lakhs (15.90 lakhs –28.39 lakhs) in 2017. India was estimated to have around 87.58 (36.45 – 172.90) thousand new HIV infections in 2017, showing new HIV infection decline by 85% since the peak of 1995 and by 27% between 2010-2017 [4].
HIV causes a wide spectrum of diseases and it is undoubtedly a multisystem disorder, but the ophthalmic disease does affect 70-80% of the patients with HIV infection. Various studies have shown that about 40-45% of the HIV infected patients have some or the other ophthalmic manifestations. Lifetime cumulative rate of at least one abnormal ocular lesion in HIV positive patient is 52%–100% in different studies [5].
Though most HIV infected patients live in developing countries; there are only a few reports on ophthalmic manifestations of HIV from the developing countries of the world [6]. Ophthalmic manifestations of HIV infection are diverse. Both anterior and posterior segments of the eye can be involved and it may even lead to blindness [7].
Keratoconjunctivitis sicca or dry eye occurs in later stages of the disease in 10 -20% of the patients. An abnormal Rose Bengal staining and Schirmer’s test is invariably detected in these patients. The cause of dry eye in HIV patients is complex. Combined effects of HIV-mediated inflammation and destruction of the lacrimal and salivary glands and direct HIV infection of the conjunctiva is the proposed mechanism [7].
As per literature there are very few studies in which they tried to correlate the severity of dry eye with CD4 count especially in North-western part of India.[7] Therefore, present study was planned to see the correlation between level of CD4 count with the severity of dry eye in HIV seropositive patients.
MATERIAL AND METHODS
Study Design, Settings and Participants
It was a hospital based cross-sectional study conducted over a period of one year from June 2018 to May 2019 in ophthalmology department of a tertiary care teaching hospital in Himachal Pradesh, India. All HIV-positive patients between 18 to 50 year of age group, registered at the ART centre and referred to Ophthalmology OPD for ocular complaints and asymptomatic patients from ART centre were selected randomly for the study. Patient with confounding factors and co morbidities like diabetes, corneal scars, lid abnormalities, contact wearers, SJS, arthritis, any other connective tissue disorder; patients who were already on treatment for DES, oral contraceptive pills, pregnant females and those taking any medications like antidepressants, antihistaminics, anxiolytics which can independently cause dry eye and seriously ill patients who were not able to cooperate for ophthalmological examination were excluded from the study. Total 346 HIV patients were examined but after considering inclusion and exclusion criterias 120 participants were finally included in our study. Every patient was on Highly Active Antiretroviral Therapy (HAART).
Data Collection
After taking written informed consent from the study subjects, data was collected in a predesigned, pre-tested, semi-structured interview schedule in which socio-demographic profile like age, gender, occupation, duration of ART, duration of disease etc were collected. After taking history as per proforma, each patient has undergone detailed ophthalmological examination in the following sequence:
Dry Eye Questionnaire - Ocular Surface Disease Index Score (OSDI): OSDI questionnaire was administered to all patients and by a single examiner. To those who were non conversant in English, the questions were explained to the patients in their local language. The OSDI questionnaire has 12 items, with each question given a score ranging from 0 (none of the time) to 4 (all of the time). The final score was calculated by multiplying the sum of all the scores by 25 and then dividing the total by the number of questions answered. Scores range from 0 to 100 with 0–12 representing normal, 13–22 representing mild DED, 23–32 representing moderate DED, and ≥33 representing severe DED [8,9]
Slit Lamp Biomicroscopy: Detailed evaluation from anterior segment to posterior segment was done. Relevant to our study detailed evaluation of lid. Eye lashes, conjuctiva, cornea, sclera, tear film height, lens was done
TBUT (Tear Film Break Up Time): Tear break-up time was performed by moistening a fluorescein strip with sterile non preserved saline and applying it to the inferior tarsal conjunctiva. After several blinks, the tear film was examined using a broad beam of the slit-lamp biomicroscope with a cobalt blue filter. The time lapse between the last blink and the appearance of the first randomly distributed dark discontinuity in the fluorescein -stained tear film is the tear break-up time. Break-up times less than 20 seconds was considered abnormal.This procedure was repeated three times on both eyes[8-10]
Schirmer-1 Test Without Anaesthesia: The Schirmer test was performed by placing a narrow filter-paper strip in the inferior cul-de-sac. Aqueous tear production was measured by the length in millimeters that the strip wets during the test period, generally 5 minutes. Test was performed with eyes closed. Serin et al. suggested that administering the Schirmer test with the patient’s eyes closed produces less variable results and greater repeatability [11]. While an isolated abnormal result can be nonspecific, serially consistent low results are highly suggestive of aqueous deficiency [9,12,13]. Severity grading was done as follows; >15 mm/5 min (Normal); 10-15 mm/5min (Mild Dry Eye);5-9 mm/5min (Moderate Dry Eye) and <5 mm/5min (Severe Dry Eye)
Schirmers Test 1 With Anaesthesia: The Schirmer test with anesthesia, also referred to as a basic secretion test, has been reported to give more variable results than the Schirmer test done without anesthesia. If topical anesthesia is applied, excess fluid should be gently removed from the cul-de-sac prior to insertion of the filter paper. This test is performed after 15 minutes of Schirmer’s test 1. After putting topical proparacaine drops, schirmer’s strip was applied as for Schirmer’s test 1. Results noted down after 5 minutes. <6mm/5min was considered abnormal and >6 mm of wetting after 5 minutes was considered normal
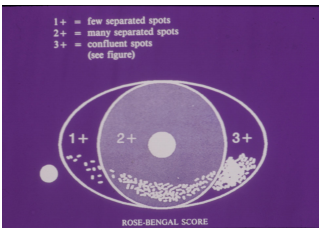
Rose Bengal Staining: Rose Bengal staining was done and graded as van bitzerveld scoring. Rose Bengal score > 4 was considered abnormal and < 4 was considered normal. Maximum score was 9. Intensity scored in 2 exposed nasal conjunctival zones and cornea. It was started after putting anaesthetic drop to avoid irritation as this stain is slightly toxic to epithelial cells [8,9]
Posterior segment examination was also performed in every patient. Those patients who were found to have abnormalities other than dry eye were treated accordingly.
Statistical Analysis
Data were analyzed and statistically evaluated using SPSS software, version 17 (Chicago II, USA). Quantitative data was expressed in mean, standard deviation while qualitative data were expressed in percentage. Statistical differences between the proportions were tested by chi square test or Fisher’s exact test. Spearman correlation coefficient was used to see the correlation between two quantitative variables. ‘P’ value less than 0.05 was considered statistically significant.
Figure 1: Rose-Bengal Scoring System for Ocular Surface Staining
Ethical Issues
All participants were explained about the purpose of the study. Confidentiality was assured to them along with informed written consent. The study was approved by the Institutional Ethical Committee
RESULTS
Out of 120 patients, 67 were males (55.8%) and 33 were females (44.2%). In 40 (33.3%) patients, CD4 count was > 500 cells/mm3 were, in 50 (41.7%) patients it was between 200 to 500 cells/mm3 and in 30 (25%) patients, CD4 cell count was <200 cells/mm3.
OSDI score was found to be positive for dry eye in 67 patients (56%). Out of 40 patients with CD4 Count > 500 cells/mm3 OSDI was abnormal in 21 (52.5%) patients, in patients with CD4 count between 200 to 500 cells/mm3 OSDI score was abnormal in 27 (54.0%) patients while in patients with CD4 count <200 cells/mm3 OSDI score was abnormal in 11 (36.7%) patients. However, trend for mild and severe dry eye cases have shown that patients severe dry eye were increasing as CD4 cell count deceases but, this association was found statistically not significant (p= 0.24) (table 1).
TBUT (Tear Film Breakup Time) was normal in 124 (51.7%) eyes while in 116 (48%) eyes TBUT was abnormal. In patients with CD4 Count > 500 cells/mm3, between 200 to 500 cells/mm3 and <200 cells/mm3 TBUT <5 seconds was seen in 2.5%, 5.0% and 10.0% patients respectively. This association was found statistically significant (p = 0.04) (table 2).
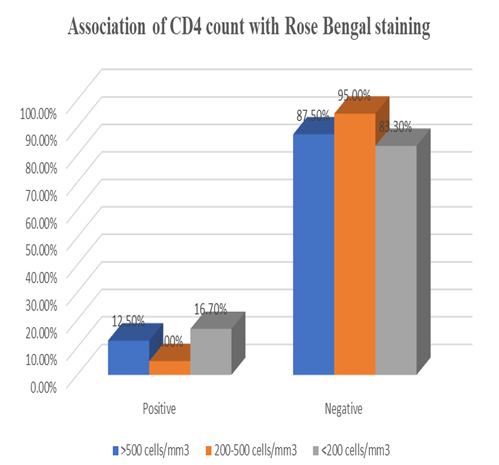
Figure 2: Association of CD4 Count with Rose Bengal Staining
Table 1: Association of CD4 count with OSDI score
OSDI score
>500 cells/mm3 (n = 40)
200-500 cells/mm3 (n = 50)
<200 cells/mm3 (n = 30)
p-value
No.
%
No.
%
No.
%
0-12 (Normal)
19
47.5
23
46.0
11
36.7
0.76
13-22 (Mild dry eye)
12
30.0
16
32.0
11
36.7
0.34
23-32 (Moderate dry eye)
6
15.0
7
14.0
4
13.3
0.12
>33 (severe dry eye)
3
7.5
4
8.0
4
13.3
0.24
Schirmer-1 test with anaesthesia was found abnormal in 81 (33.7%) eyes while on Schirmer-1 test without anaesthesia 31% (75) were found to be abnormal. No significant association was seen between Schirmer-1 test without anaesthesia with CD4 count but CD4 count was significantly associated Schirmer-1 test with anaesthesia (p<0.001) (Table 3).
On rose Bengal staining 25 (10.4%) eyes were found positive. Highest number of positive eyes (16.7%) were seen in patients with CD4 count <200 cells/mm3 compare to patients with CD4 Count > 500 cells/mm3 (12.5%) and CD4 count between 200 to 500 cells/mm3 (5.0%). This association was also found statistically significant (p = 0.04) (Figure 1).
On using spearman correlation coefficient, significant mild positive correlation was seen between CD4 count and Schirmer-1 test without anaesthesia score (r value = 0.23; p-value<0.001), Schirmer -1 with anaesthesia score (r value = 0.22; p-value<0.001), Tear Film Breakup Time (TBUT) (r value = 0.28; p value<0.01) but no correlation was seen with OSDI score (r value = -0.01, p-value = 0.83).
Table 2: Association of CD4 count with Tear Film Breakup Time (TBUT)
Tear Film Breakup Time (TBUT)
>500 cells/mm3
200-500 cells/mm3
<200 cells/mm3
p-value
No.
%
No.
%
No.
%
>20 sec (Normal)
54
67.5
56
56.0
14
23.3
<0.001
10-20 sec (Mild dry eye)
15
18.8
19
19.0
24
40.0
0.13
5-9 (Moderate dry eye)
9
11.2
20
20.0
16
26.7
0.22
<5 sec (severe dry eye)
2
2.5
5
5.0
6
10.0
0.04
Table 3: Association of CD4 Count with Schirmer -1 Test with and Without Anaesthesia
Parameters
>500 cells/mm3
200-500 cells/mm3
<200 cells/mm3
p-value
No.
%
No.
%
No.
%
Schirmer-1 test without anaesthesia
>15mm/5 min (Normal)
62
77.5
66
66.0
37
61.7
0.14
10-15 mm/5 min (Mild dry eye)
10
12.5
20
20.0
15
25.0
0.28
5-9 mm/5 min (Moderate dry eye)
5
6.2
12
12.0
6
10.0
0.31
<5 mm/5 min (severe dry eye)
3
3.8
2
2.0
2
3.3
0.15
Schirmer-1 test with anaesthesia
>6mm/5 min (Normal)
63
78.8
70
70.0
26
43.3
<0.001
<6 mm/5 min (abnormal)
17
21.2
30
30.0
34
56.7
DISCUSSION
Kerato-conjunctivitis sicca has been reported as one of the most common anterior segment manifestations. Various studies conducted on normal population have shown that the prevalence of dry eye ranges between 10% and 20% [7,14-16]
The etiology of dry eye disease in HIV patients is usually thought to be due to HIV-mediated lymphocytic infiltration of the lacrimal gland. This leads to the destruction of lacrimal acini and the ductal system, as well as direct conjunctival damage [17]. Dry eye can also be due to blepahritis in these patients, pathogenesis of which explained as reduced ability in these patients to control normal flora and more complex changes in cutaneous glands of eyelids. Meibomitis has been the causative factor in lipid layer dysfunction in these patients [18]. The resulting keratoconjunctivitis contributes to a chronic inflammatory state, further promoting cytokine secretion, destruction and dysfunction of the lacrimal gland, and loss of tear production [19]. Since HIV has been isolated from retina, it is believed that ocular complication results either from a general decrease of host immunity as seen with decreasing CD4 cell count more likely, direct ocular infection by HIV through the blood-aqueous barrier and/or blood-retinal barrier [17,20]
In our study, association between OSDI and CD4 cell count for detecting the dry eye severity as disease progresses was not found to be statistically significant (p>0.005), but the fact that 56% of our study subjects had dry eye symptoms should not be ignored and it clearly indicates the magnitude of problem in these HIV/AIDS patients. To the best of my knowledge no study has been done so far which has used OSDI score for diagnosing dry eye in PLWHA.
In our study it was observed that in patients with CD4 Count > 500 cells/mm3, between 200 to 500 cells/mm3 and <200 cells/mm3 TBUT <5 seconds was seen in 2.5%, 5.0% and 10.0% patients respectively. This association was found statistically significant (p= 0.04). Finding of our study were in concordance with Gowda HT et al. [7] in which patients with CD4 count of 101-500 cells/mm3 the tear film break up time was <10 s only in 12 eyes (27.27%). In patients with 0-100 cells/mm3 and >500 cells/mm3 only 20.59% and 4.5% of the eyes had dry eye. Our results were also comparable with Mathebula et al. they have also found increasing dry eye cases and disease severity is increasing tested with TBUT [21]
In present study, Schirmer-1 test with anaesthesia was found abnormal in 81 (33.7%) eyes while on Schirmer-1 test without anaesthesia 31% (75) were found to be abnormal. No significant association was seen between Schirmer-1 test without anaesthesia with CD4 count but CD4 count was significantly associated Schirmer-1 test with anaesthesia (p<0.001). Similar significant association was found in study by Gowda HT et al. [7].
On rose Bengal staining 25 (10.4%) eyes were found positive. Highest number of positive eyes (16.7%) were seen in patients with CD4 count <200 cells/mm3 compare to patients with CD4 Count > 500 cells/mm3 (12.5%) and CD4 count between 200 to 500 cells/mm3 (5.0%). This association was also found statistically significant (p = 0.04). In study by Gowda HT et al[7], Rose Bengal test in the count of 0-100 cells/mm3, only 7 eyes were positive for Rose Bengal staining which constitutes 20.59% and in 101-500 cells/mm3 only 29.55% eyes were positive. But, with count of >500 cells/mm3 100% were negative (p = 0.018). This shows concordance with our study.
CONCLUSION
Present study concluded that positive and statistically significant correlation was found between CD4 cell count and Schirmer-1 test without and with anaesthesia and TBUT only. Hence dry eye in PLWHA should not be looked down upon and should be treated for the same. More studies with larger sample size are needed to see the ocular involvement and correlation of CD-4 cell count with dry eye severity for treatment and better visual prognosis.
Acknowledgement
We are grateful to all the participants of the study.
REFERENCE
World Health Organisation. "Factsheet no 360: HIV/AIDS." WHO, 2015. http://www.who.int/mediacentre/factsheets /fs360/en/.
Acharya P.K. et al. "Ocular manifestations in patients with HIV infection/AIDS who were referred from the art centre Hassan Karnataka India." Journal of Clinical and Diagnostic Research, vol. 6, no. 10, 2012, p. 1756.
World Health Organization. "AIDS epidemic update." WHO, 2017–2018.
National AIDS Control Organization. "Annual report 2017–18." Ministry of Health and Family Welfare, 2018.
Sharma R.L. et al. "Ocular manifestations in human immunodeficiency virus/acquired immuno deficiency syndrome patients and their correlation with CD4+ T-lymphocyte count." Annals of Tropical Medicine and Public Health, vol. 5, no. 5, 2012, p. 474.
Hodge W.G. et al. "Ocular opportunistic infection incidences among patients who are HIV positive compared to patients who are HIV negative." Ophthalmology, vol. 105, no. 5, 1998, pp. 895–900.
Gowda H.K. et al. "Correlation of CD4 count and severity of dry eye disease in human immunodeficiency virus positive patients." International Journal of Scientific Study, vol. 3, 2015, pp. 68–71.
"TFOS DEWS II definition and classification report." Acta Ophthalmologica, vol. 96, no. S261, 2018, pp. 136–140.
"Introduction to the report of the International Dry Eye Workshop 2007." The Ocular Surface, vol. 5, no. 2, 2007, pp. 69–70. https://www.sciencedirect.com/science/ article/pii/S1542012412700782.
Akobiec F.A. et al. Albert & Jakobiecs Principles & Practice of Ophthalmology. W.B. Saunders Company, 2008.
Serin D. et al. "A simple approach to the repeatability of the Schirmer test without anesthesia: eyes open or closed?" Cornea, vol. 26, no. 8, 2007, pp. 903–906.
Krachmer J. et al. Cornea. Elsevier, 2017.
Listed N.A. "The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye Workshop." The Ocular Surface, vol. 5, no. 2, 2007, pp. 75–92.
Sharma M. et al. "Ocular manifestations in patients attending antiretroviral therapy centre at a tertiary care hospital in Himachal Pradesh India." The Indian Journal of Medical Research, vol. 147, no. 5, 2018, p. 496.
Hashemi H. et al. "Prevalence of dry eye syndrome in an adult population." Clinical & Experimental Ophthalmology, vol. 42, no. 3, 2014, pp. 242–248.
Sahai A. and Malik P. "Dry eye: prevalence and attributable risk factors in a hospital-based population." Indian Journal of Ophthalmology, vol. 53, no. 2, 2005, pp. 87–91.
Stewart M.W. "Human immunodeficiency virus and its effects on the visual system." Infectious Disease Reports, vol. 4, no. 1, 2012.
Jeng B.H. et al. "Anterior segment and external ocular disorders associated with human immunodeficiency virus disease." Survey of Ophthalmology, vol. 52, no. 4, 2007, pp. 329–368.
Biswas J. et al. "Ocular lesions in AIDS: a report of first two cases in India." Indian Journal of Ophthalmology, vol. 43, no. 2, 1995, p. 69.
Amsalu A. et al. "Ocular manifestation and their associated factors among HIV/AIDS patients receiving highly active antiretroviral therapy in Southern Ethiopia." International Journal of Ophthalmology, vol. 10, no. 5, 2017, p. 776.
Mathebula S.D. and Makunyane P.S. "Ocular surface disorder among HIV and AIDS patients using antiretroviral drugs." African Vision and Eye Health, vol. 78, no. 1, 2019, pp. 1–7.
None
None
None
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Applied Medical Sciences and Research open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Advertisement
Recommended Articles
Research Article
Evaluation of Serum Heat Shock Protein 70 as a Diagnostic Biomarker for Ectopic Pregnancy: A Comparative Case-Control Study
Hala Ahmed Atiya,
Ayla Khedher Ghalib
Published: 28/02/2026
Download PDF
Cite
x
APA
Atiya, H. A. & Ghalib, A. K. (2026). Evaluation of Serum Heat Shock Protein 70 as a Diagnostic Biomarker for Ectopic Pregnancy: A Comparative Case-Control Study. Himalayan Journal of Applied Medical Sciences and Research, 7(1), 1-5.
MLA
Atiya, Hala A. and Ayla K. Ghalib. "Evaluation of Serum Heat Shock Protein 70 as a Diagnostic Biomarker for Ectopic Pregnancy: A Comparative Case-Control Study." Himalayan Journal of Applied Medical Sciences and Research 7.1 (2026): 1-5.
Chicago
Atiya, Hala A. and Ayla K. Ghalib. "Evaluation of Serum Heat Shock Protein 70 as a Diagnostic Biomarker for Ectopic Pregnancy: A Comparative Case-Control Study." Himalayan Journal of Applied Medical Sciences and Research 7, no. 1 (2026): 1-5.
Harvard
Atiya, H. A. and Ghalib, A. K. (2026) 'Evaluation of Serum Heat Shock Protein 70 as a Diagnostic Biomarker for Ectopic Pregnancy: A Comparative Case-Control Study' Himalayan Journal of Applied Medical Sciences and Research 7(1), pp. 1-5.
Vancouver
Atiya HA, Ghalib AK. Evaluation of Serum Heat Shock Protein 70 as a Diagnostic Biomarker for Ectopic Pregnancy: A Comparative Case-Control Study. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Assessing First Trimester Maternal Serum Pentraxin-3 Levels in Primary Unexplained Recurrent Pregnancy Loss: A Case-Control Study
Raniah Ibrahim Khaleel Yaseen,
Israa Hashim Abdalkareem
Published: 28/02/2026
Download PDF
Cite
x
APA
Yaseen, R. I. K. & Abdalkareem, I. H. (2026). Assessing First Trimester Maternal Serum Pentraxin-3 Levels in Primary Unexplained Recurrent Pregnancy Loss: A Case-Control Study. Himalayan Journal of Applied Medical Sciences and Research, 7(1), 1-6.
MLA
Yaseen, Raniah I. K. and Israa H. Abdalkareem. "Assessing First Trimester Maternal Serum Pentraxin-3 Levels in Primary Unexplained Recurrent Pregnancy Loss: A Case-Control Study." Himalayan Journal of Applied Medical Sciences and Research 7.1 (2026): 1-6.
Chicago
Yaseen, Raniah I. K. and Israa H. Abdalkareem. "Assessing First Trimester Maternal Serum Pentraxin-3 Levels in Primary Unexplained Recurrent Pregnancy Loss: A Case-Control Study." Himalayan Journal of Applied Medical Sciences and Research 7, no. 1 (2026): 1-6.
Harvard
Yaseen, R. I. K. and Abdalkareem, I. H. (2026) 'Assessing First Trimester Maternal Serum Pentraxin-3 Levels in Primary Unexplained Recurrent Pregnancy Loss: A Case-Control Study' Himalayan Journal of Applied Medical Sciences and Research 7(1), pp. 1-6.
Vancouver
Yaseen RIK, Abdalkareem IH. Assessing First Trimester Maternal Serum Pentraxin-3 Levels in Primary Unexplained Recurrent Pregnancy Loss: A Case-Control Study. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jan;7(1):1-6.
Download PDF
Research Article
Patent Ductus Arteriosus Medical Closure and Associated Co-morbidities in Premature Infants in Sulaymaniyah Neonatal Intensive Care Unit
Adil Ali Zainel,
...
Mustafa Elias Abdulqader3
Published: 28/02/2026
Download PDF
Cite
x
APA
Zainel, A. A., Rasheed, S. R. & Abdulqader3, M. E. (2026). Patent Ductus Arteriosus Medical Closure and Associated Co-morbidities in Premature Infants in Sulaymaniyah Neonatal Intensive Care Unit. Himalayan Journal of Applied Medical Sciences and Research, 7(1), 1-5.
MLA
Zainel, Adil A., Sirwa R. Rasheed and Mustafa E. Abdulqader3. "Patent Ductus Arteriosus Medical Closure and Associated Co-morbidities in Premature Infants in Sulaymaniyah Neonatal Intensive Care Unit." Himalayan Journal of Applied Medical Sciences and Research 7.1 (2026): 1-5.
Chicago
Zainel, Adil A., Sirwa R. Rasheed and Mustafa E. Abdulqader3. "Patent Ductus Arteriosus Medical Closure and Associated Co-morbidities in Premature Infants in Sulaymaniyah Neonatal Intensive Care Unit." Himalayan Journal of Applied Medical Sciences and Research 7, no. 1 (2026): 1-5.
Harvard
Zainel, A. A., Rasheed, S. R. and Abdulqader3, M. E. (2026) 'Patent Ductus Arteriosus Medical Closure and Associated Co-morbidities in Premature Infants in Sulaymaniyah Neonatal Intensive Care Unit' Himalayan Journal of Applied Medical Sciences and Research 7(1), pp. 1-5.
Vancouver
Zainel AA, Rasheed SR, Abdulqader3 ME. Patent Ductus Arteriosus Medical Closure and Associated Co-morbidities in Premature Infants in Sulaymaniyah Neonatal Intensive Care Unit. Himalayan Journal of Applied Medical Sciences and Research. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community
Vishal Dhatwalia,
Swati Chandel
Published: 10/12/2024
Download PDF
Cite
x
APA
Dhatwalia, V. & Chandel, S. (2024). Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research, 5(2), 1-5.
MLA
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5.2 (2024): 1-5.
Chicago
Dhatwalia, Vishal and Swati Chandel. "Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community." Himalayan Journal of Applied Medical Sciences and Research 5, no. 2 (2024): 1-5.
Harvard
Dhatwalia, V. and Chandel, S. (2024) 'Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community' Himalayan Journal of Applied Medical Sciences and Research 5(2), pp. 1-5.
Vancouver
Dhatwalia V, Chandel S. Bones in Balance: Awareness of Rickets and Nutritional Deficiencies Among the Hamirpur Community. Himalayan Journal of Applied Medical Sciences and Research. 2024 Jul;5(2):1-5.
Sharma, S., Rajput, G. & Gupta, D. (2021). Correlation of CD4 Count and severity of dry eye in People Living with HIV and AIDS (PLWHA). Himalayan Journal of Applied Medical Sciences and Research, 2(2), 1-5.
MLA
Sharma, Sheetal, G.C. Rajput and Dalip Gupta. "Correlation of CD4 Count and severity of dry eye in People Living with HIV and AIDS (PLWHA)." Himalayan Journal of Applied Medical Sciences and Research 2.2 (2021): 1-5.
Chicago
Sharma, Sheetal, G.C. Rajput and Dalip Gupta. "Correlation of CD4 Count and severity of dry eye in People Living with HIV and AIDS (PLWHA)." Himalayan Journal of Applied Medical Sciences and Research 2, no. 2 (2021): 1-5.
Harvard
Sharma, S., Rajput, G. and Gupta, D. (2021) 'Correlation of CD4 Count and severity of dry eye in People Living with HIV and AIDS (PLWHA)' Himalayan Journal of Applied Medical Sciences and Research 2(2), pp. 1-5.
Vancouver
Sharma S, Rajput G, Gupta D. Correlation of CD4 Count and severity of dry eye in People Living with HIV and AIDS (PLWHA). Himalayan Journal of Applied Medical Sciences and Research. 2021 Jul;2(2):1-5.