Patients and Methods
This prospective cohort study was conducted from August 2024 to July 2025 at Al-Kadhimiya Teaching Hospital and Imam Ali Hospital, Baghdad, Iraq. The study aimed to evaluate the risk factors and complications associated with femoral shaft fractures in adult patients, with particular emphasis on venous thromboembolism and bleeding outcomes. The study population consisted of young adult patients presenting with compound fractures of the lower limb long bones caused by missile injuries.
Inclusion Criteria
Patients were eligible for inclusion if they met the following criteria:
Acute traumatic injury
Compound fracture(s) of a single lower limb long bone (Gustilo type IIIA or IIIB) caused by missile injuries
Admission and management in the orthopedic ward for at least 10 days
Isolated orthopedic injuries without involvement of other body systems
No documented history of chronic medical comorbidities prior to injury
Exclusion Criteria
Patients were excluded if they met any of the following criteria:
Associated contralateral lower limb injuries and/or spinal injuries
Newly diagnosed comorbidities during hospital admission
Pelvic or spinal fractures
Previous injury to the affected limb or history of deep vein thrombosis
Sampling and Data Collection
The study sample included 33 trauma patients with compound fractures of one lower limb long bone caused by missile injuries, involving the femur, tibia, or both ipsilateral bones. Data were collected by the researcher through direct patient follow-up using a structured data collection form.
The patients’ ages ranged from 16 to 48 years and all participants were male. All patients were initially admitted through the emergency department. Initial evaluation was performed according to the Advanced Trauma Life Support (ATLS) protocol and secondary survey, which confirmed isolated orthopedic injuries.
During emergency management, patients received appropriate antibiotics, analgesics and fluid resuscitation. Laboratory investigations and radiological assessments were performed on admission.
Following emergency stabilization, patients were transferred to the orthopedic ward for further assessment and management. All patients underwent urgent wound debridement and external fixation. Fractures were classified according to the Gustilo classification system and only type IIIA and IIIB injuries were included in the study.
External fixation was applied to the femur, tibia, both bones, or as spanning fixation, depending on the injury pattern. External fixation was used either as temporary stabilization before conversion to internal fixation or as definitive treatment. Management included single or multiple sessions of wound debridement with repeated clinical evaluation.
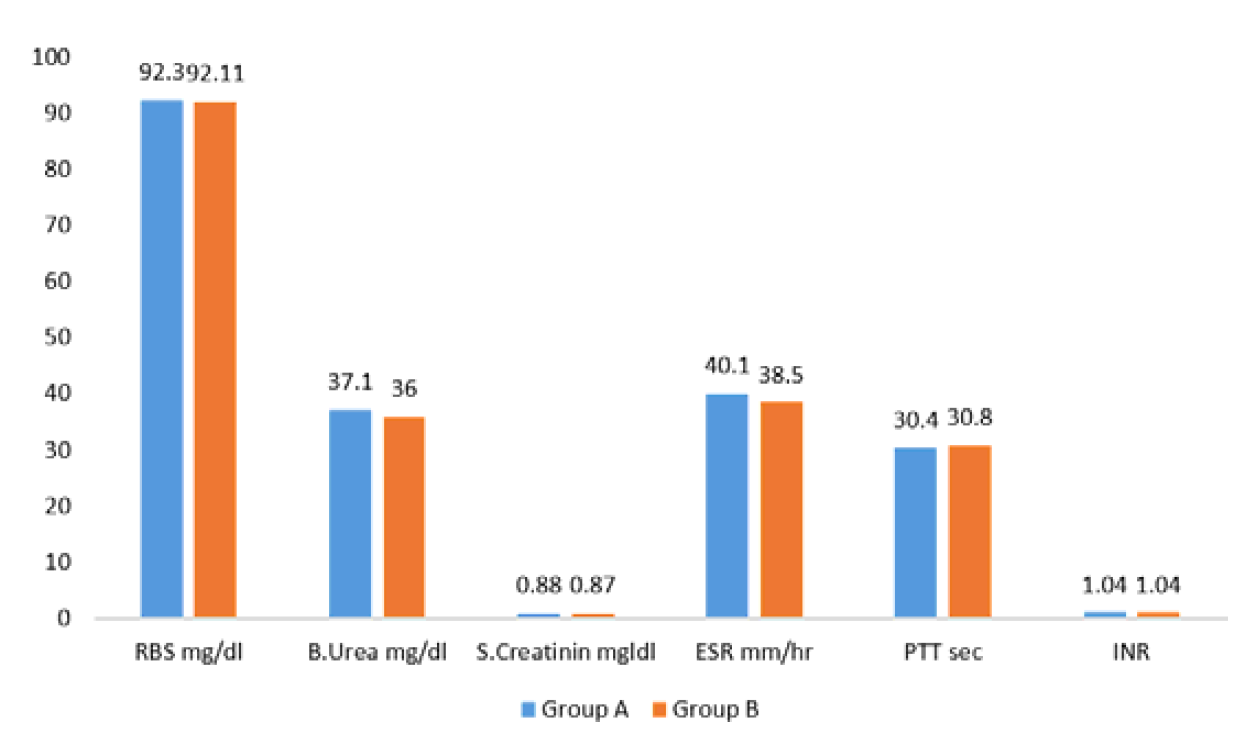
All patients received one or more units of blood transfusion during hospitalization. Emergency laboratory investigations on admission included hemoglobin level, random blood glucose, blood urea and serum creatinine. Follow-up laboratory tests were performed on the second day of admission and during the remaining hospital stay, including complete blood picture, fasting blood glucose, renal function tests and coagulation profile (PT, PTT and INR).
Study Groups and Thromboprophylaxis
Patients were managed by multiple orthopedic surgeons from different units within the department. According to the treating surgeons’ clinical decisions, patients were divided into two groups:
Pharmacological prophylaxis consisted of subcutaneous enoxaparin 4000 IU once daily, initiated within 12 hours after urgent surgical intervention. A baseline platelet count was obtained before starting therapy. Additional baseline assessments included patient body weight, coagulation profile, renal function tests and complete blood picture.
Clinical Monitoring and Follow-Up
All patients underwent daily clinical assessment for signs and symptoms of deep vein thrombosis, including:
Leg swelling
Redness
Local warmth
Tenderness
Monitoring for complications of pharmacological prophylaxis was also performed daily, with particular attention to bleeding from the wound site or other anatomical sites.
Between the 10th and 14th day of admission, all patients underwent Doppler ultrasonography of the lower limbs as a screening test for venous thrombosis.
Data were collected throughout the hospitalization period, which ranged from 10 to 14 days.
Outcome Measures
Patients were followed for the following outcome measures:
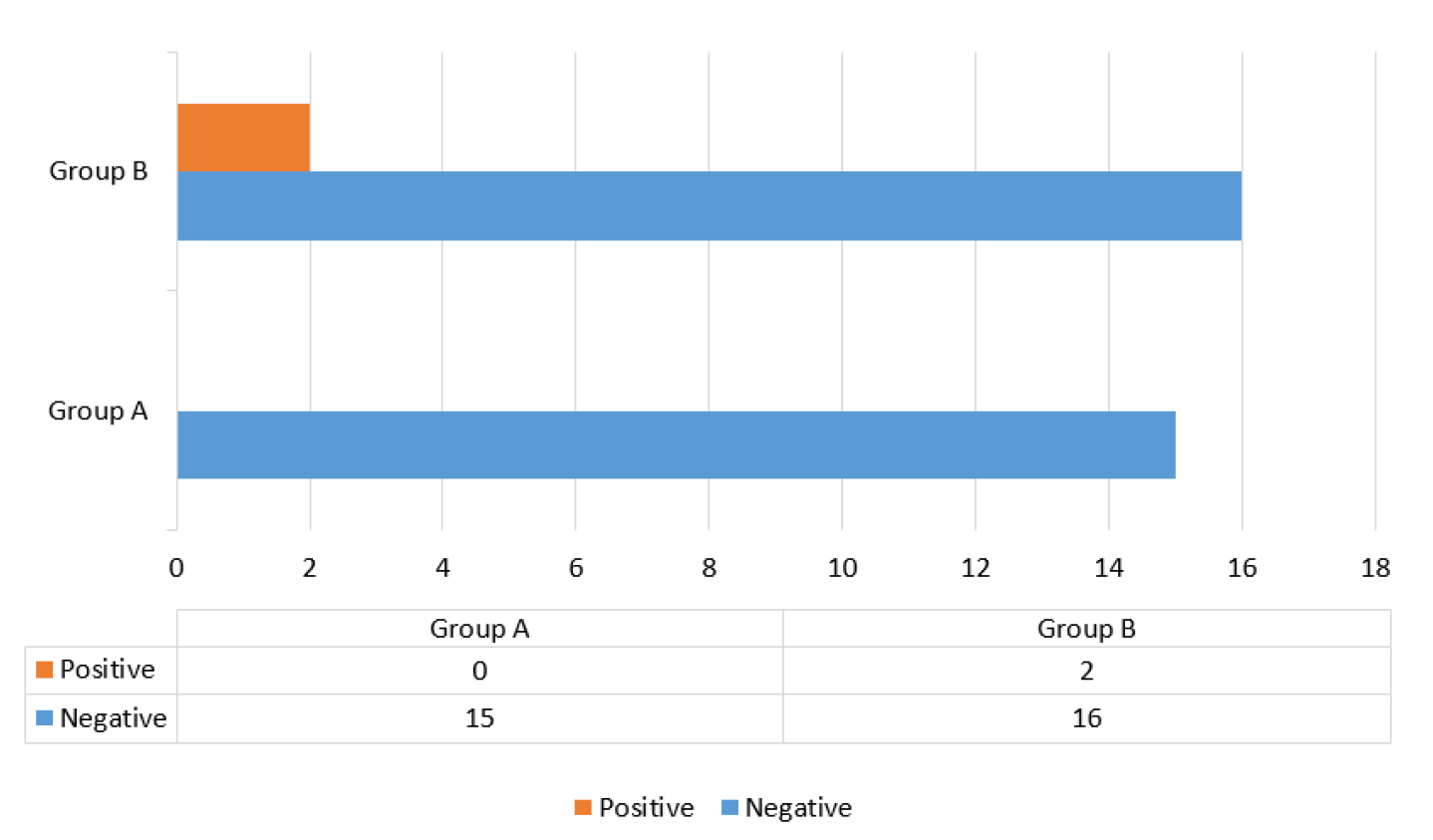
Evidence of deep vein thrombosis, based on clinical signs and symptoms and Doppler ultrasound findings
Evidence of bleeding tendency, defined as bleeding from sites other than the wound and/or abnormal coagulation profile results
Following completion of orthopedic management, patients were either transferred to the plastic surgery unit for further care, discharged home, or referred to nearby hospitals for continued treatment.
Statistical Analysis
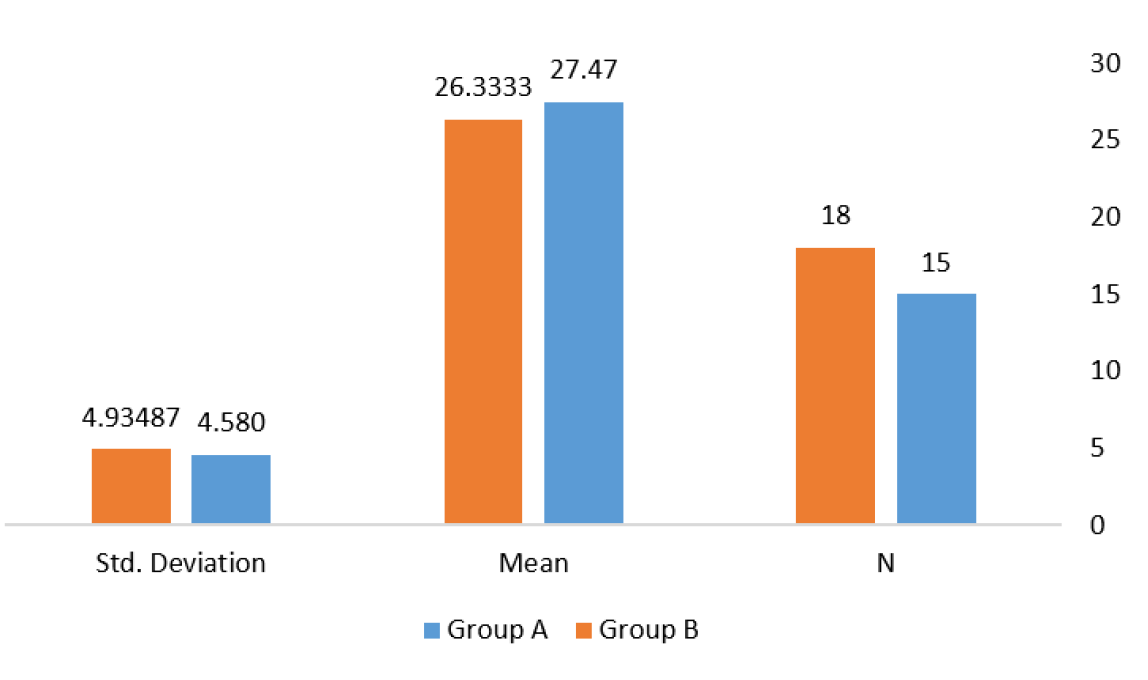
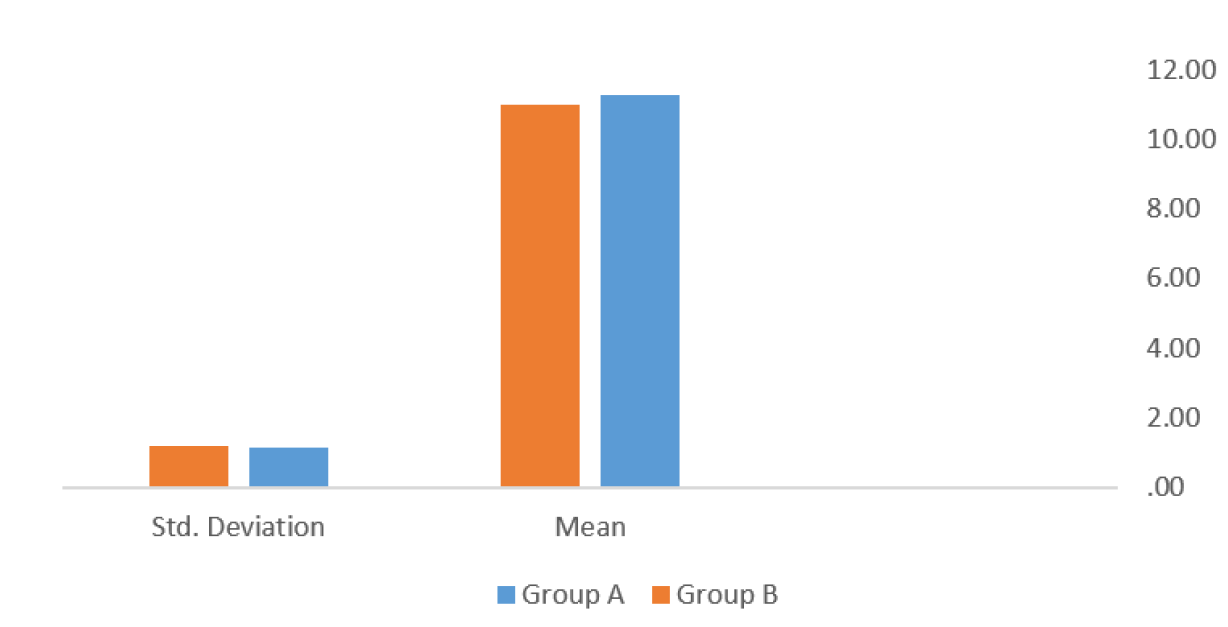
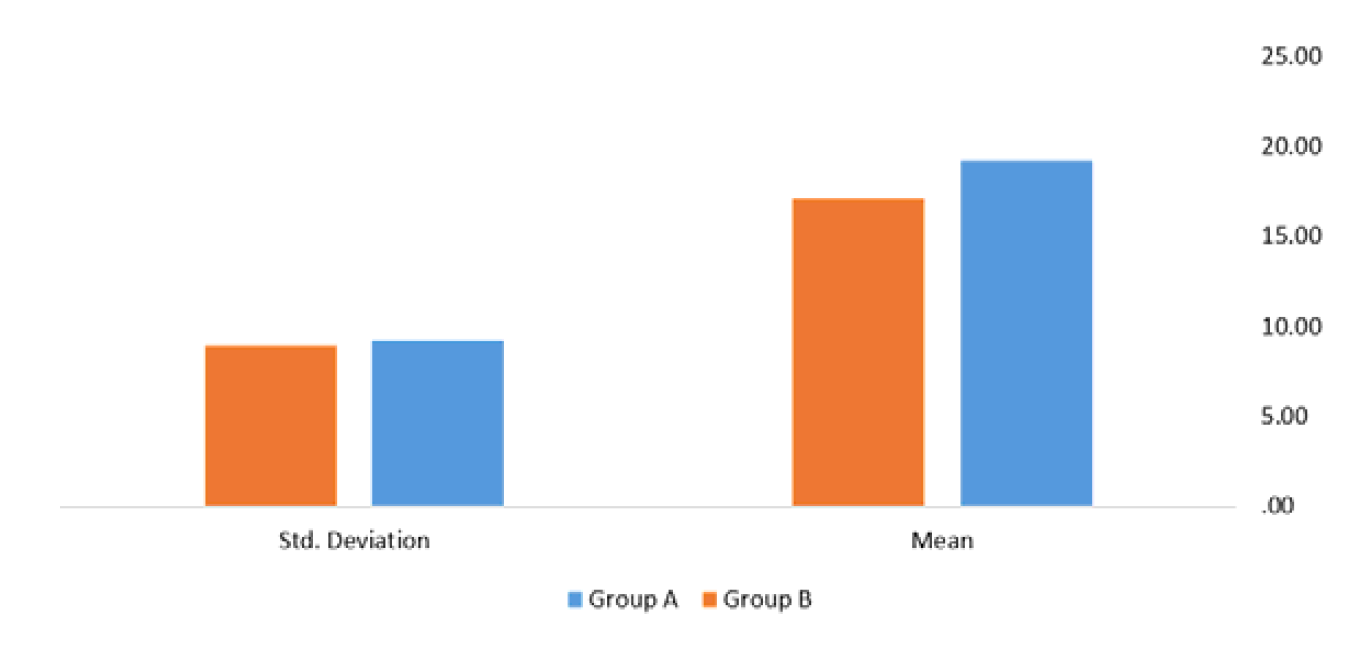
All collected data were entered and analyzed using computerized statistical software. Descriptive statistics were expressed as mean and standard deviation for continuous variables and as frequencies and percentages for categorical variables.
Comparative analyses were performed using Student’s t-test for parametric data and Fisher’s exact test for categorical variables. A p-value of less than 0.05 was considered statistically significant. Results were presented in the form of tables and graphs.