We present a 32 year old male with ocular trauma by sharp object resulting in corneal laceration and iris prolapse. This case shows importance of early diagnosis, proper wound repair and value of early postoperative visual rehabilitation.
Keywords
Open globe injury
Iris prolapse
Visual acuity
Globe Repair
INTRODUCTION
Open Globe injury is a common ophthalmic emergency. It is a leading cause of blindness. We should examine the patient thoroughly and treat the patient as early as possible. Preoperative care must include antibiotics, analgesics and no manipulation to globe.[1] In cases of open globe injuries when there is iris prolapse, making a paracentesis opposite to the area of the prolapse is advised; this is followed by injection of a minimal amount of a viscoelastic and gentle repositioning of the iris using an iris sweep. Injecting excessive viscoelastic can result in increased pressure and additional iris prolapse. An important point in such cases is to avoid inadvertent incarceration of the iris into the suture as well as to avoid cutting the iris, except in cases in which it is frankly necrotic or epithelialized because the iris tissue can be used for future reconstruction.[2]
CASE
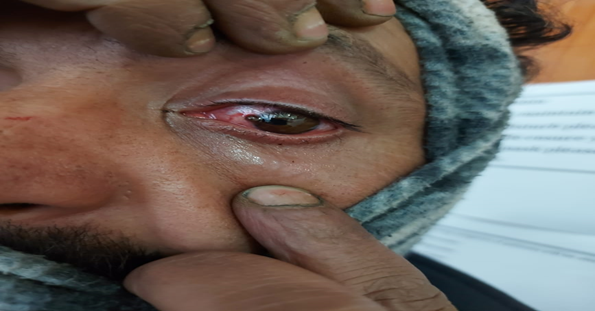
A 32-year-old male presented to emergency department with history of trauma to left eye by sharp object, ocular pain and dimunition of vision. On examination, visual acuity in right eye was 6/6 and left eye 6/24. There was circumciliary congestion, limbal laceration extending from 9o clock position to 10o clock position with iris prolapsed (Figure 1). Posterior segment could not be examined.
Repair was done under local anaesthesia. A protective eye shield was placed and the
patient was sent for X-ray; no intraocular foreign body was detected. The patient then was given tetanus immunization, antiemetics, analgesics and intravenous broad-spectrum antibiotics and prepared for globe repair under local anaesthesia. Laboratory tests included complete blood count, liver function tests, kidney function tests and all were within normal limits.
Figure 1: Patient with traumatic prolapsed of left iris.
Repair of the right globe rupture was done under LA, which included sterilization of conjunctiva by povidone-iodine eye drops. No scleral extension of the wound was found. The reparative steps in this case followed those mentioned previously: creation of a paracentesis opposite the area of prolapse, injection of minimal viscoelastic, and iris sweep. Before any corneal sutures are placed, the iris may prolapse again after the sweep and so placing a few sutures before sweeping may be necessary. The prolapsed iris was viable and was reposited by iris spatula. Limbal sutures were placed using 10/0 Nylon sutures.
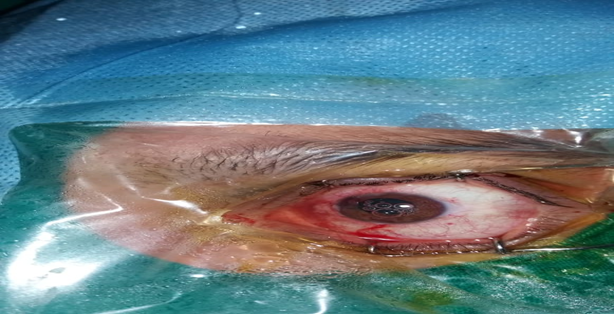
In the first postoperative visit, the eye was slightly congested with periorbital ecchymosis and conjunctival chemosis. Anterior chamber was formed and no signs of wound leakage or infection were found (Figure 2). Best corrected visual acuity after 4 weeks was 6/9.
Figure 2: Patient on first post-operative visit.
DISCUSSION
Ocular trauma is a common ophthalmic emergency.[3] Rapid and accurate diagnosis of ruptured globe is mandatory to savevisual acuity and prevent further damage of the eye although diagnosis of occult globe rupture may be challenging.[3] Alarming signs that raise the suspicion of globe rupture include: hyphema, sub-conjunctival hemorrhage, abnormally deep or abnormally shallow anterior chamber, distorted pupil or irido-dialysis, low intraocular pressure, uveal tissue exposure and limitation of ocular motility.[4] If globe injury is suspected, emergency ophthalmic consultation mustbe taken after stabilization of the general condition of the patient. Ocular manipulation must be avoided.
Funding: No funding sources
Conflict of interest: None declared
Ethical approval: The study was approved by the Institutional Ethics Committee of Regional Hospital, Himachal Pradesh
Bord, S. P., and J. Linden. "Trauma to the Globe and Orbit." Emergency Medicine Clinics of North America, vol. 26, no. 1, 2008, pp. 97-123. DOI: 10.1016/j.emc.2007.11.006.
Pulmonary Function Test (PFT) and 6 Minutes’ Walk Test Findings among Interstitial Lung Diseases (ILDS) Patients in a Tertiary Care Hospital
Vir Singh
Published: 27/11/2021
Download PDF
Cite
x
APA
Singh, V. (2021). Pulmonary Function Test (PFT) and 6 Minutes’ Walk Test Findings among Interstitial Lung Diseases (ILDS) Patients in a Tertiary Care Hospital. Himalayan Journal of Community Medicine and Public Health, 2(2), 1-3.
MLA
Singh, Vir. "Pulmonary Function Test (PFT) and 6 Minutes’ Walk Test Findings among Interstitial Lung Diseases (ILDS) Patients in a Tertiary Care Hospital." Himalayan Journal of Community Medicine and Public Health 2.2 (2021): 1-3.
Chicago
Singh, Vir. "Pulmonary Function Test (PFT) and 6 Minutes’ Walk Test Findings among Interstitial Lung Diseases (ILDS) Patients in a Tertiary Care Hospital." Himalayan Journal of Community Medicine and Public Health 2, no. 2 (2021): 1-3.
Harvard
Singh, V. (2021) 'Pulmonary Function Test (PFT) and 6 Minutes’ Walk Test Findings among Interstitial Lung Diseases (ILDS) Patients in a Tertiary Care Hospital' Himalayan Journal of Community Medicine and Public Health 2(2), pp. 1-3.
Vancouver
Singh V. Pulmonary Function Test (PFT) and 6 Minutes’ Walk Test Findings among Interstitial Lung Diseases (ILDS) Patients in a Tertiary Care Hospital. Himalayan Journal of Community Medicine and Public Health. 2021 Jul;2(2):1-3.
Download PDF
Research Article
Understanding Endocrine Health: Public Knowledge of Thyroid Disorders in Women's Reproductive Health in Shimla District
Kajal ,
...
Raghav Nirula
Published: 05/04/2025
Download PDF
Cite
x
APA
None, K., None, P. & Nirula, R. (2025). Understanding Endocrine Health: Public Knowledge of Thyroid Disorders in Women's Reproductive Health in Shimla District. Himalayan Journal of Community Medicine and Public Health, 6(1), 1-4.
MLA
None, Kajal, Priya and Raghav Nirula. "Understanding Endocrine Health: Public Knowledge of Thyroid Disorders in Women's Reproductive Health in Shimla District." Himalayan Journal of Community Medicine and Public Health 6.1 (2025): 1-4.
Chicago
None, Kajal, Priya and Raghav Nirula. "Understanding Endocrine Health: Public Knowledge of Thyroid Disorders in Women's Reproductive Health in Shimla District." Himalayan Journal of Community Medicine and Public Health 6, no. 1 (2025): 1-4.
Harvard
None, K., None, P. and Nirula, R. (2025) 'Understanding Endocrine Health: Public Knowledge of Thyroid Disorders in Women's Reproductive Health in Shimla District' Himalayan Journal of Community Medicine and Public Health 6(1), pp. 1-4.
Vancouver
Kajal K, Priya P, Nirula R. Understanding Endocrine Health: Public Knowledge of Thyroid Disorders in Women's Reproductive Health in Shimla District. Himalayan Journal of Community Medicine and Public Health. 2025 Jan;6(1):1-4.
Download PDF
Research Article
Dyspepsia, An Overview With Diet
Ashish Tajne Toofan Chakravarty
Published: 20/08/2025
Download PDF
Cite
x
APA
Toofan Chakravarty, A. T. (2021). Dyspepsia, An Overview With Diet. Himalayan Journal of Community Medicine and Public Health, 2(4), 1-1.
MLA
Toofan Chakravarty, Ashish Tajne. "Dyspepsia, An Overview With Diet." Himalayan Journal of Community Medicine and Public Health 2.4 (2021): 1-1.
Chicago
Toofan Chakravarty, Ashish Tajne. "Dyspepsia, An Overview With Diet." Himalayan Journal of Community Medicine and Public Health 2, no. 4 (2021): 1-1.
Harvard
Toofan Chakravarty, A. T. (2021) 'Dyspepsia, An Overview With Diet' Himalayan Journal of Community Medicine and Public Health 2(4), pp. 1-1.
Vancouver
Toofan Chakravarty AT. Dyspepsia, An Overview With Diet. Himalayan Journal of Community Medicine and Public Health. 2021 Iss;2(4):1-1.
Download PDF
Research Article
Road Traffic Accidents: A Global and Indian Perspective on Trends, Burden, Risk Factors and Preventive Strategies
Tushar ,
...
Rahul Rai
Published: 05/04/2025
Download PDF
Cite
x
APA
None, T., Paul, D. & Rai, R. (2025). Road Traffic Accidents: A Global and Indian Perspective on Trends, Burden, Risk Factors and Preventive Strategies. Himalayan Journal of Community Medicine and Public Health, 6(1), 1-2.
MLA
None, Tushar, Dharam Paul and Rahul Rai. "Road Traffic Accidents: A Global and Indian Perspective on Trends, Burden, Risk Factors and Preventive Strategies." Himalayan Journal of Community Medicine and Public Health 6.1 (2025): 1-2.
Chicago
None, Tushar, Dharam Paul and Rahul Rai. "Road Traffic Accidents: A Global and Indian Perspective on Trends, Burden, Risk Factors and Preventive Strategies." Himalayan Journal of Community Medicine and Public Health 6, no. 1 (2025): 1-2.
Harvard
None, T., Paul, D. and Rai, R. (2025) 'Road Traffic Accidents: A Global and Indian Perspective on Trends, Burden, Risk Factors and Preventive Strategies' Himalayan Journal of Community Medicine and Public Health 6(1), pp. 1-2.
Vancouver
Tushar T, Paul D, Rai R. Road Traffic Accidents: A Global and Indian Perspective on Trends, Burden, Risk Factors and Preventive Strategies. Himalayan Journal of Community Medicine and Public Health. 2025 Jan;6(1):1-2.
Gupta, A., Negi, S. & Kumar, J. (2022). Case Report: Repair of an Open Globe Injury. Himalayan Journal of Community Medicine and Public Health, 3(1), 1-2.
MLA
Gupta, Atul, Shaloo Negi and Jitender Kumar. "Case Report: Repair of an Open Globe Injury." Himalayan Journal of Community Medicine and Public Health 3.1 (2022): 1-2.
Chicago
Gupta, Atul, Shaloo Negi and Jitender Kumar. "Case Report: Repair of an Open Globe Injury." Himalayan Journal of Community Medicine and Public Health 3, no. 1 (2022): 1-2.
Harvard
Gupta, A., Negi, S. and Kumar, J. (2022) 'Case Report: Repair of an Open Globe Injury' Himalayan Journal of Community Medicine and Public Health 3(1), pp. 1-2.
Vancouver
Gupta A, Negi S, Kumar J. Case Report: Repair of an Open Globe Injury. Himalayan Journal of Community Medicine and Public Health. 2022 Jan;3(1):1-2.