Ongoing pandemic of COVID –19 which is a major challenge for public health and clinical medicine, has spread throughout the world, affecting more than 100 million people and more than 2 million deaths. COVID-19 is caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), single stranded RNA viruses. COVID -19 mainly involve respiratory system with cardinal symptoms include fever, cough and shortness of breath. Other symptoms include muscle pain, anorexia, chest tightness, loss of taste and smell [1]. However, presently gastrointestinal manifestations of COVID -19 is increasingly being recognized [2]. Pancreatic involvement had been seen with other viral infections but acute viral pancreatitis due to COVID -19 is not a well recognized entity. Here, we report a case of acute pancreatitis in COVID -19 infections.
Case History
A 35 year old female presented to our emergency department with chief complaints of severe epigastric pain for last 1 day which is radiating to back. Pain is associated with nausea and vomiting. There is some improvement in severity of pain on banding forward. There is no history of fever, cough and shortness of breath. She denied any history of alcoholism, smoking and similar complaint in past. She refused for any drug history in past. On physical examination, she was afebrile, respiratory rate of 24/ min, had tachycardia (pulse rate of 104 bpm) with oxygen saturation of 95 % on room air. On abdominal examination there is severe epigastric tenderness with soft non- distended abdomen. Other systemic examination was within normal limits.
Her laboratory investigations revealed the following serum amylase 899 U/L, lipase 710 U/L, total leucocyte count 11500, Hb 14.1 g/dl, platelet count 1,90,000, serum aspartate aminotransferase 66 U/l, alanine aminotransferase 46 U/L, alkaline phosphatase 99 U/L, bilirubin total 0.9 mg/dl, blood urea nitrogen 27mg/dl, creatinine 0.5mg/dl, Na + 140 meq/l, K+ 3.5 meq/l, Ca 2+ 9.5mg/dl, phosphorus 3.5mg/dl. CT scan
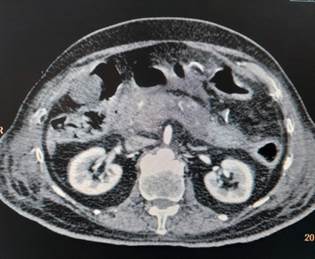
Figure 1: Axial Contrast-Enhanced CT Image Showing Bilateral Kidneys and Abdominal Viscera

Figure 2: BH: Abdominal CT (Axial) – Kidneys and Bowel Loops Visualized
of abdomen (Figure 1) showed bulky/ enlarged and heterogenous pancreas with non-enhancing necrotic areas within it. Tail is poorly visualized (likely necrotic). Peripancreatic fat stranding with peripancreatic fluid is noted – features suggestive of acute necrotizing pancreatitis. As a routine protocol for admission in intensive care unit during this covid era, her nasopharyngeal and oropharyngeal swab was sent for COVID-19 testing by reverse transcriptase polymerase chain reaction (RT-PCR) which came out to be positive. Diagnosis of acute viral pancreatitis, COVID-19 induced, was kept. She was admitted in COVID-19 isolation ward and treated symptomatically with bowl rest, intravenous fluids, analgesia and empirical antibiotics. She was managed conservatively and discharged in hemodynamically stable condition after 1 week.


