Background: Wound dehiscence is multifactorial in etiology, conditioned by local and systemic, as well as pre-, intra-, and post-operative factors. The present study was done to evaluate the effect of various Co-morbidities on abdominal wound dehiscence After Midline Laparotomy. Material & Method: The present cross-sectional study was conducted in the Department of General Surgery, IGMC, Shimla, Himachal Pradesh from June 2018 to December 2019. The patients who require midline laparotomy were randomized into Group 1 and Group 2. The patients in Group 1 underwent closure of rectus sheath with conventional continuous closure technique and in Group 2 underwent closure with interrupted X suture technique. A total of 100 patients were included in each group. Results: In this study there were 79% males and 21% females in Group -1 while there were 89% males and 11% females in Group 2. In group 1, mean age was 47.08 years and SD ± 15.81. In group 2, mean age was 45.65 years and SD ± 14.93 In Group 1, out of 100 patients wound dehiscence occurred in 32 cases while in Group 2, out of 100 patients wound dehiscence occurred in 6 cases. In Group 1, 20 patients were anemic, 7 patients were diabetics, 20 patients had uremia, 75 patients had hypoalbuminemia, 62 patients had chest infection. In Group 2, 13 patients were anemic, 6 patients were diabetics, 19 patients had uremia, 67 patients had hypo-albuminemia and 39 patients had chest infection. Conclusion: Besides technique of closure, various factors like malnutrition, cough, intra-peritoneal sepsis, wound infection, wound gaping, abdominal distension are significant predictors of burst abdomen. Patients with these risk factors require more attention and in presence of these factors, the risk of wound dehiscence can be reduced considerably by using interrupted X-suture technique.
Keywords
Co-Morbidities
Wound Dehiscence
Continuous Suture Technique
Interrupted X Suture Technique
INTRODUCTION
Abdominal wound dehiscence (AWD) is the separation of different layers of an abdominal wound before complete healing has taken place [1]. Incidence of post-laparotomy wound dehiscence/burst abdomen varies from center to center. While the incidence of wound dehiscence has been reported as 1–3% in most centers across the world, some centers in India have recorded an incidence rate of burst abdomen as high as 10–30%. Wound dehiscence is multi-factorial in etiology, conditioned by local and systemic, as well as pre-, intra-, and post-operative factors. Post-operative complete wound dehiscence, being an unfortunate and also a serious complication, is associated with high morbidity and mortality rate despite the most sophisticated intensive care these patients receive today. Wound dehiscence is multifactorial in etiology, conditioned by local and systemic, as well as pre-, intra-, and post-operative factors [2-5].
Despite advances in peri-operative care and suture materials, incidence and mortality rates in regard to abdominal wound dehiscence have not significantly changed over the past decades. This may be attributable to increasing incidences of risk factors within patient populations outweighing the benefits of technical achievements. Several mainly retrospective studies have been performed to identify risk factors for this complication, often presenting conflicting results [6]. Various factors are significant predictors of burst abdomen.
According to many studies, various Risk factors for wound dehiscence or burst abdomen are elderly, diabetes malnutrition, obesity, anemia, jaundice, hypo-protenemia, intra-abdominal malignancy, intra-abdominal sepsis and many others [7,8].
Against this backdrop, present study was conducted to evaluate the effect of various co-morbidities on abdominal wound dehiscence after Midline Laparotomy in a tertiary care hospital wound dehiscence in a tertiary care hospital.
Aims and Objective
To evaluate the effect of various co-morbidities on abdominal wound dehiscence after Midline Laparotomy in a tertiary care hospital.
MATERIALS AND METHODS
Source of Data
This study was conducted on 200 patients undergoing midline laparotomy in the Department of General Surgery, Indira Gandhi Medical College, Shimla from June 2018 to December 2019. Patients were selected who require midline laparotomy either as emergency or elective procedure.
Inclusion Criteria:
Patients aged 18-75 years, requiring laparotomy
Gender: Both male and female
Patients who require surgery with midline incision either as emergency or elective procedure
All patients giving written informed consent for enrollment in study
Exclusion Criteria
Patients below 18 years and above 75 years
Patients aged 18-75 years with immuno-compromised state, on chemotherapy/immunotherapy, long term steroids
Patients who died within 10 days following midline laparotomy
Patients undergoing Re-Laparotomy
Study Design:
It was a prospective randomized comparative study on 200 patients who were divided into two groups 100 each by sealed envelope method and they were randomized accordingly.
Group A: Closed by suturing the rectus sheath using Polydioxanone suture 1-0 (PDS) in conventional continuous layer suturing technique.
Group B: Closed by suturing the rectus sheath using Polydioxanone suture 1-0 (PDS) in interrupted –X suture technique.
Study procedure
Closure of midline abdominal wound by Continuous layer suturing technique with polydioxanone No 1 (PDS) suture.
Method of Collection of Data
Pre-Operative Evaluation: The patients were assessed preoperatively with clinical history, physical examination, biochemical and radiological evaluations. A detailed Performa was filled with the following details:
Details of patient age, sex, address, CR No., Date of Admission, Date of discharge
Brief History
General Physical Examination
Details of Operative Procedure
Date of surgery
Operation
Indication
Findings
Closure Technique
Patients included in the study undergone following investigations:
Abdomen X-Ray (AP View in Erect and Supine Position)
Ultrasound Abdomen/CT
Electrocardiography (ECG)
Intra-Operative Technique
After parts painted and draped, midline incision was given and abdomen was opened in layers. Once the pathology dealt, abdominal drains placed rectus sheath was closed either by continuous or interrupted X suture technique by PDS 1-0 RB as per group allocation.
Suture Material
PDS 1-0 Round body was used in both groups.
Technique of Continuous Closure
Continuous Closure Technique: Continuous closure, performed using PDS 1-0 RB, care being taken to place each bite 1.5-2 cm from linea alba edge with successive bites being placed 1 cm from each other. The linea Alba was gently approximated without strangulation.
Interrupted X-Closure
Interrupted X-closure performed using PDS 1-0 RB as large bite being taken outside as 2 cm from the cut edge of linea alba. The needle emerged on other side from inside out diagonally 2 cm from the edge and 4 cm above or below the first bite. This strand subsequently crossed or looped around the free end of suture and continued outside in diagonally at 90o to the first diagonal. The two-end tied just tight enough to approximate the edge of linea alba taking care not to include omentum or bowel between the edges. This created two X like crosses- one on the surface and another deep to linea alba. The next X- suture placed 1 cm away from the previous one. Henceforth, in a 14 cm long wound, 3 X-sutures was applied.
Post-Operative Evaluation
In post-operative period, patients examined daily, kept nil per oral and on par-enteral fluids till bowel recover and assessed for the following parameters:
Cough
Discharge
Abdominal Distension
Drain output
Wound Gaping
Wound Dehiscence
Anemia
Broad Spectrum antibiotic coverage was given and changed as per culture sensitivity of wound discharge. Daily dressing was done.
In asymptomatic patients with no wound infection, gaping and wound dehiscence, skin sutures removed on 10th post-operative day.
Follow Up
Regular follow up done up-to 7th, 10th and 14th day. During follow up above mentioned parameters assessed.
Statistical Analysis
The present study was carried out in a randomized prospective manner and statistical analysis of the data done at the end of the study using appropriate statistical tests depending upon the variables. Quantitative data was presented as mean and range as appropriate. For normally distributed data, mean was compared using T-test. For discrete categorical data, number and percentage were calculated. Chi-Square tests or Fisher’s exact tests were applied for categorical data. All statistical tests were two sided. A p value of <0.05 was considered to indicate statistical significance. Analysis was conducted using Epi-Info version 7.2.3.1.
OBSERVATION AND RESULTS
The study was conducted in the Department of General Surgery, Indira Gandhi Medical College and Hospital, Shimla, Himachal Pradesh from June 2018 to December 2019. A total of 200 patients were included in the study.
The patients were randomized into two groups, Group 1 and Group 2. The patients included in Group 1 underwent closure of rectus sheath with conventional continuous closure technique and patients included in Group 2 underwent closure of rectus sheath with interrupted X suture technique. A total of 100 patients were included in each group.
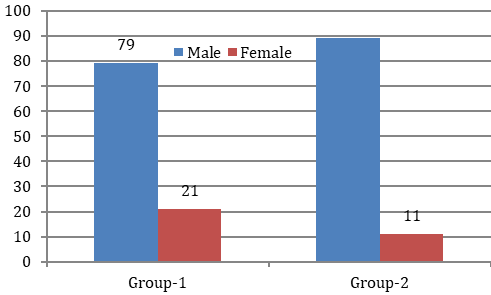
In this study there were 79% males and 21% females in Group 1 while there were 89% males and 11% females in Group 2. This data when analyzed by the Chi-Square test, gave a p value of 0.0537 which was not significant which means that both Groups were comparable with respect to the sex distribution of the patient (Table 1 and Figure 1).
In group 1, age of the patients varied from 18–75 years with a mean age 47.08 years and SD ± 15.81. In group 2, age of the patients varied from 18-75 years with a mean age of 45.65 years and SD ± 14.93. On analysis by the student T-test, it shown that the age variation between the two groups was statistically insignificant with a p value of 0.51. Thus, both the groups were comparable with respect to the age distribution of the patients (Table 1).
Figure 1: Gender distribution of Study Participants
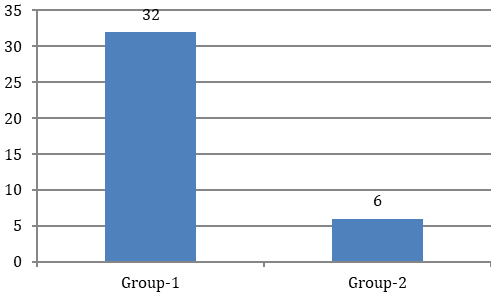
Figure 2: Wound Dehiscence in both groups
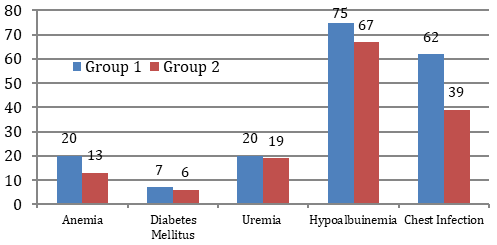
Figure 3: Various Co-Morbidities among study participants
Table 1: Age & Gender distribution of Study Participants
Variables
Group 1
Group 2
P-Value
Gender
Male
79%
89%
0.0537
Female
21%
11%
Age
Mean age
47.08± 15.81
45.65± 14.93
0.51
Wound dehiscence
Yes
32
6
0.00001
No
68
94
Table 2: Various Co-Morbidities among study participants
Study Group
Anemia
(Hb<10 mg/dl)
Diabetes Mellitus
Uremia
(>50 mg/dl)
Hypoalbuinemia
(< 3.5 mg/dl)
Chest Infection
Group 1
20
7
20
75
62
Group 2
13
6
19
67
39
Total
33
13
39
142
101
In Group 1, out of 100 patients wound dehiscence occurred in 32 cases while in Group 2, out of 100 patients wound dehiscence occurred in 6 cases. The difference of wound dehiscence in two groups was statistically significant (Table 1 and Figure 2).
In Group 1, 20 patients were anemic, 7 patients were diabetics, 20 patients had uremia, 75 patients had
Table 4: Association of various co-morbidities with Wound Dehiscence
Pre-Operative Parameters
Wound Dehiscence
Total
P-Value
Yes
No
frequency
%
frequency
%
Technique Of Closure
Group 1
32
32.00
68
68.00
100
0.00001
Group 2
6
06.00
94
94.00
100
Anemia
Group 1
10
50.00
10
50.00
20
0.05
Group 2
2
15.38
11
84.62
13
Hypo-Albuminemia
Group 1
28
37.33
47
60.00
70
0.0000
Group 2
6
8.96%
61
91.04
67
Uremia
Group 1
7
35.00%
13
65.00
20
0.08
Group 2
2
10.53%
17
89.47
19
Diabetes Mellitus
Group 1
0
0.00
7
100.00
7
0.0000
Group 2
0
0.00
6
100.00
6
Leukocytosis
Group 1
19
46.34
22
53.66
41
0.0007
Group 2
4
11.11%
32
88.89
36
Cough
Group 1
27
43.55
35
56.45
62
0.0004
Group 2
4
10.26%
35
89.74
39
Emergency Procedure
Group 1
26
28.89
64
71.11
90
0.0000
Group 2
6
6.38
88
93.62
94
hypoalbuminemia, 62 patients had chest infection. In Group 2, 13 patients were anemic, 6 patients were diabetics, 19 patients had uremia, 67 patients had hypoalbuminemia, 39 patients had chest infection (Table 2 and Figure 3).
Total sample size of study was 200 and out of which 38 (19%) developed wound dehiscence in post-operative period. Stratified analysis was performed for the significant predictor to better understand the efficacy of the two methods under different conditions.
Out of 200 patients, 100 patients were randomized under the conventional continuous closure method and 100 patients underwent interrupted X suture technique of abdomen closure. It was observed that in Group1 who underwent continuous closure technique, 32 (32%) patient developed burst, while in Group 2 who underwent interrupted X suture technique 6 (6%) patients developed wound dehiscence. On analysis Chi-Square test it was observed that variation between the two groups was statistically significant with a p value of <0.00001.
In Group 1, 50% (10) of patients who were anemic develop wound dehiscence and in Group 2, 15.38% (2) patients who were anemic develop wound dehiscence.
Adequate nutrition is essential to support cellular activity, timely recovery and wound healing. Hypoalbuminemia is very important risk factor for development of burst abdomen. In Group 1, 37.33% (28) of patients who were having hypoalbuminemia developed wound dehiscence and in Group 2, 8.96% (6) patients who were having hypoalbuminemia developed wound dehiscence.
In present study wound dehiscence was associated with uremia. Out of 200 patients, 39 patients were having uremia, out of 39 patients 20 patients were in continuous group and 19 patients were in interrupted X suture group. 7 (35%) patients in Group 1 and 2 (10.53%) patients in Group 2 developed wound dehiscence.
Diabetes is a systemic disease and causes immunosuppression. Diabetic patients have delayed wound healing. In this study 13 out of 200 patients were diabetic. Out of 13 diabetic patients, 7 patients were in Group 1 and 6 patients were in Group 2. Although there is correlation between wound infection and wound dehiscence associated with diabetes mellitus but in present study patients had good glycemic control and none in both groups developed wound dehiscence.
Patients having septicemia have relatively poor wound healing. In current study 41 patients in Group 1 and 36 patients in Group 2 having leukocytosis at the time of presentation. Out of which 19 (46.34%) patients in Group 1 and 4 (11.11%) patients in Group 2 developed the wound dehiscence.
Presence of cough at time of hospital admission and early post-operative period was analyzed as a predictor in outcome of burst abdomen. Out of 200 cases 101 (50.50%) presented with cough or developed cough in early post-operative period. In Group 1 out of 62 patients, 43.55% (27) patients having cough developed wound dehiscence and in Group 2 out of 39 patients, 10.26% (4) patients had cough and developed wound dehiscence. On analysis Chi-Square Test it showed that variation between the two groups was statistically significant with a p value of 0.000413.
In this study out of 200 patients, the surgical site infection and wound gaping was present in 85 (42.5%) patients. Out of 85, 38 (44.7%) patients developed wound dehiscence in post-operative period. On statistical analysis the p value on Fisher Exact test was 0.00001. Thus, surgical site infection was a highly significant predictor of wound dehiscence.
Abdominal distension is associated with burst abdomen. In this study abdominal distension was present in 30 (15%) patients. Out of 30 patients who developed abdominal distension, 12 (40%) patients had abdominal wound dehiscence in post-operative period. Out of 170 patients who did not have abdominal distension, only 26 (15.29%) patients developed wound dehiscence. On statistical analysis the p value on Chi-Square was 0.001. Thus, abdominal distension was a highly significant predictor of wound dehiscence.
Type of procedure i.e. emergency or elective procedure is associated with burst abdomen. In this study 184 (92%) patients operated in emergency and 16 (8%) operated in elective setting. 38 (19%) developed wound dehiscence. 32 (84.21%) developed wound dehiscence in emergency procedure and 6 (15.78%) patients developed wound dehiscence in elective procedure.
DISCUSSION
Abdominal wound dehiscence defined as post-operative wound separation that involves all the layers of abdomen wall. Dehiscence of an abdominal wound may be partial or complete.
The present study was performed at Indira Gandhi Medical College & Hospital, Shimla, HP, to compare the rate of abdominal wound dehiscence in continuous versus interrupted X suture technique for abdominal wall closure in midline laparotomy.
In current study 200 patients enrolled and all underwent midline laparotomy and a total of 38 (19%) patients had wound dehiscence, out of which 32% (32 out of 100) patients in conventional continuous suture group developed wound dehiscence, while 6% (6 out of 100) patients in the interrupted X suture group developed wound dehiscence. The difference of wound dehiscence in two groups was statistically significant.
In 2017, Ahi et al. [8] conducted a prospective randomized study of conventional continuous versus Interrupted-X type versus Hughes Far and Near interrupted abdominal fascial closure in surgical patients to prevent burst abdomen. They took 90 patients, 19 (21%) of 90 patients develop burst in the post-operative period. 11 (36.7%) of 30 patients in continuous arm developed burst, 4 out of 30 (13.3%) patients in Interrupted-X arm and 4 out of 30 (13.3%) patients in Huges Far and Near arm developed burst abdomen. On statistical analysis it is found significant (p=0.011) and the results obtained in the current study were comparable to this study.
In present study in Group 1, 10 out of 20 patients who were anemic develop wound dehiscence and in Group 2, 2 out of 13 patients who were anemic develop wound dehiscence. On statistical analysis, Chi-Square test, it showed that variation between two groups was insignificant. In 2012, Agarwal et al. [9] did a randomized control trial comparing Interrupted –X and conventional continuous closure in surgical and gynecological patients to prevent burst abdomen. Burst occurred in 10 (9.80 %) of 102 patients with anaemia. 19 (7.72 %) of 246 patients without anaemia had burst. Thus, on statistical analysis the anaemia was not a detrimental factor in the development of burst abdomen.
In current study, Group 1 who underwent continuous wound closure, 37.33% (28) of patients who were having hypoalbuminemia developed wound dehiscence and in Group 2 who underwent interrupted X suture 63 wound closure, 8.96% (6) patients who were having hypoalbuminemia developed wound dehiscence. On statistical analysis, it is found that, poor nutrition in form of hypoalbuminemia is significant risk factor in wound dehiscence. In 2014, study by Ramneesh Garg et al. [10], pre-operative hypoalbuminemia was noted in 15 patients out of 50 emergency exploratory laparotomies. Among 6 patients who developed wound dehiscence 4 of them had preoperative hypoalbuminemia. On statistical analysis, it is found to be significant with p value of 0.037. This significance of hypoalbuminemia in influencing wound dehiscence coincides with most of studies in literature and present study.
In this study wound dehiscence was associated with uremia. Out of 200 patients, 39 patients were having uremia, out of 39 patients 20 patients were in continuous group and 19 patients were in interrupted X suture group. 7 (35%) out of 20 patients in group 1 and 2 (10.53%) out of 19 patients in group 2 developed wound dehiscence. on Chi Square test p value was 0.747 which was not significant. In 2017, study by Ahi [8], 20 patients had uraemia, out of these 5 (25.0%) patients developed burst abdomen. Remaining 70 patients were found to be non - uremic, out of these 14 (20.0%) patients developed 64 burst abdomens. The analysis of above was not statistically significant (p=0.629) and this study was comparable to present study.
In present study 13 out of 200 patients were diabetic. Out of 13 diabetic patients, 7 patients were in Group 1 and 6 patients were in Group 2. Out of 187 patients who were not diabetic, 38 developed burst abdomens. Although there is correlation between wound infection and wound dehiscence associated with diabetes mellitus but in this study, patients had good glycemic control and none in both groups having diabetes mellitus developed wound dehiscence. On statistical analysis the fisher exact test the p value was 0.683 which was not significant. In 2012, Agarwal et al. [9] did a randomized control trial comparing Interrupted –X and conventional continuous closure. In their study, nine of the 348 patients included in the study were known diabetics. One (11.11 %) of these developed bursts in the postoperative period. Of those not having diabetes, 28 (8.26 %) developed burst. On statistical analysis two-sided Fisher’s exact p value was 0.547, which was not significant showing results similar to those obtained in the current study.
In current study of 200 cases, 101 (50.50%) presented with cough or developed cough in early post-operative period. Out of 101, 43.55% (27) patients in Group 1 and 10.26% (4) patients in Group 2 had cough and developed wound dehiscence. On analysis, Chi-Square Test, it showed that variation between the two groups was statistically significant with a p value of 0.000413. In 2004, Srivastava et al. [11] conducted a randomized trial, comparing continuous versus interrupted X-sutures in prevention of burst abdomen. In their study a total of 65.65% had no coughing, 2.02% had atelectasis, 17.17% had chronic obstructive airway disease (COAD), 12.12% had asthma and 3.03% had bronchopneumonia. 5.88% of patients with COAD, 8.33% of patients with asthma and 33.33% of patients with bronchopneumonia developed dehiscence thus showing that postoperative bronchopneumonia could be a significant factor in predicting a high risk of burst.
Wound infection (SSI) and wound gaping is very common after laparotomy. In present study out of 200 patients, the surgical site infection and wound gaping was present in 85 (42.5%) patients. Out of 85, 38 (44.7%) patients developed wound dehiscence in post-operative period. On statistical analysis the p value on Fisher Exact test was 0.00001. Thus, surgical site infection was a highly significant predictor of wound dehiscence. In 2012, study by Aggarwal et al. [9] Surgical site infection (SSI) was present in 57 (16.38 %) of 348 patients. Of these, 21 (36.84 %) developed burst in the postoperative period. Of those not having surgical site infection, 8 (2.75 %) developed burst abdomen postoperatively. Thus, surgical site infection was a highly significant (p=0.000) predictor of wound dehiscence.
Abdominal distension is associated with burst abdomen. In our study abdomen distension was present in 30 (15%) patients. Out of 30 patients who developed abdominal distension, 12 (40%) patients had abdominal wound dehiscence in post-operative period. Out of 170 patients who did not have abdominal distension, only 26 (15.29%) patients developed wound dehiscence. On statistical analysis the p value on Chi-Square was 0.001. Thus, abdominal distension was a highly significant predictor of wound dehiscence. In 2004, study by Srivastava et al. [11], all the cases of dehiscence of the abdominal wound had abdominal distension.
Type of procedure i.e. emergency and elective procedure is associated with burst abdomen. In current study 184 (92%) patients operated in emergency and 16 (8%) operated in elective setting. 38 (19%) developed wound dehiscence, 32 (84.21%) developed wound dehiscence in emergency procedure and 6 (15.78%) patients developed wound dehiscence in elective procedure. There was statistically significant wound dehiscence in emergency procedure group. In 2012, study by Aggarwal et al. [9], out of 234 emergency surgeries, 26 (11.11 %) patients developed burst abdomen. The risk of burst in continuous arm was 19.28 % (16/83) as opposed to 6.94 % (5/67) in interrupted X arm. In elective operations, the risk of burst in continuous arm was 7.89 % (3/38). No bursts were reported in interrupted X. Hence the wound dehiscence was statistically significant in emergency procedure showing result similar to those obtained in current study.
Finally, it has been observed that interrupted X suture techniques preferably be used in all emergency or elective laparotomy cases presenting with one or more risk factors for burst abdomen.
CONCLUSION
Wound dehiscence is associated with psychological stress to the patient and operating surgeon with increased cost of post-operative care and increased morbidity or mortality. The present study concludes that interrupted - X suture technique is better than the conventional continuous method in closure of midline laparotomy incision as the post - operative complications of wound dehiscence is found to be significantly lesser with the use of interrupted X suture technique. Although Interrupted X suture technique requires more time than the conventional continuous method but has better outcome in post-operative period. Wound dehiscence rate is more in emergency midline laparotomies as compared to elective cases. Besides technique of closure, various factors like malnutrition, cough, intra-peritoneal sepsis, wound infection, wound gaping, abdominal distension are significant predictors of burst abdomen. Patients with these risk factors require more attention and in presence of these factors, the risk of abdominal wound dehiscence can be reduced considerably by using interrupted X-suture technique.
REFERENCE
Smith, J.A.R. “Complications, prevention and management.” Clinical Surgery in General. Churchill-Livingstone, London, UK, 1999, p. 350.
Sharma, G. et al. “Comparison of suture technique (interrupted vs. continuous) with respect to wound dehiscence.” Indian Journal of Medical Sciences, vol. 72, no. 3, 31 Dec. 2020, pp. 191–94.
Singh, A. et al. “Technique of abdominal wall closure: a comparative study.” Indian Journal of Surgery, vol. 43, 1981, pp. 785–90.
Shukla, H.S. et al. “Burst abdomen and suture material: a comparison of abdominal wound closure with monofilament nylon and chromic catgut.” Indian Journal of Surgery, vol. 43, 1981, pp. 487–91.
Chowdhury S.K. and S.D. Choudhury. “Mass closure versus layer closure of abdominal wound: a prospective clinical study.” Journal of the Indian Medical Association, vol. 92, no. 7, 1 July 1994, pp. 229–32.
Van-Ramshorst, G.H. et al. “Abdominal wound dehiscence in adults: development and validation of a risk model.” World Journal of Surgery, vol. 34, no. 1, Jan. 2010, pp. 20–27.
Lakshmi G. and T.R. Ravimohan. “Post laparotomy abdominal wound dehiscence: a study in tertiary care hospital.” International Journal of Contemporary Medical Research, vol. 5, no. 11, 2018, pp. K1–K5.
Ahi K.S. et al. “Prevention of burst abdomen by interrupted closure: a comparative study of conventional continuous versus interrupted-X-type versus Hughes far-and-near interrupted abdominal fascial closure in surgical patients.” ISOR Journal, vol. 16, 2017, pp. 21–30.
Agrawal C.S. et al. “Interrupted abdominal closure prevents burst: randomized controlled trial comparing interrupted-X and conventional continuous closures in surgical and gynecological patients.” Indian Journal of Surgery, vol. 76, no. 4, Aug. 2014, pp. 270–76.
Ramneesh G. et al. “A prospective study of predictors for post laparotomy abdominal wound dehiscence.” Journal of Clinical and Diagnostic Research: JCDR, vol. 8, no. 1, Jan. 2014, p. 80.
Srivastava A. et al. “Prevention of burst abdominal wound by a new technique: a randomized trial comparing continuous versus interrupted X-suture.”
Advertisement
Recommended Articles
Research Article
Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India
Rahul Rai,
...
Tushar
Published: 05/04/2025
Download PDF
Cite
x
APA
Rai, R., Paul, D. & None, T. (2025). Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India. Himalayan Journal of Medicine and Surgery, 6(1), 1-3.
MLA
Rai, Rahul, Dharam Paul and Tushar . "Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India." Himalayan Journal of Medicine and Surgery 6.1 (2025): 1-3.
Chicago
Rai, Rahul, Dharam Paul and Tushar . "Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India." Himalayan Journal of Medicine and Surgery 6, no. 1 (2025): 1-3.
Harvard
Rai, R., Paul, D. and None, T. (2025) 'Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India' Himalayan Journal of Medicine and Surgery 6(1), pp. 1-3.
Vancouver
Rai R, Paul D, Tushar T. Clinicopathological Profile and Disease Presentation Patterns in Colorectal Cancer: A Prospective Observational Study from a Tertiary Care Center in North India. Himalayan Journal of Medicine and Surgery. 2025 Jan;6(1):1-3.
Download PDF
Research Article
Posture and Prevention: Evaluating Public Knowledge of Cervical Spondylitis in Gandhinagar, Gujarat
Nirav Oza,
Priyanka Prajapati
Published: 25/05/2025
Download PDF
Cite
x
APA
Oza, N. & Prajapati, P. (2025). Posture and Prevention: Evaluating Public Knowledge of Cervical Spondylitis in Gandhinagar, Gujarat. Himalayan Journal of Medicine and Surgery, 6(1), 1-5.
MLA
Oza, Nirav and Priyanka Prajapati. "Posture and Prevention: Evaluating Public Knowledge of Cervical Spondylitis in Gandhinagar, Gujarat." Himalayan Journal of Medicine and Surgery 6.1 (2025): 1-5.
Chicago
Oza, Nirav and Priyanka Prajapati. "Posture and Prevention: Evaluating Public Knowledge of Cervical Spondylitis in Gandhinagar, Gujarat." Himalayan Journal of Medicine and Surgery 6, no. 1 (2025): 1-5.
Harvard
Oza, N. and Prajapati, P. (2025) 'Posture and Prevention: Evaluating Public Knowledge of Cervical Spondylitis in Gandhinagar, Gujarat' Himalayan Journal of Medicine and Surgery 6(1), pp. 1-5.
Vancouver
Oza N, Prajapati P. Posture and Prevention: Evaluating Public Knowledge of Cervical Spondylitis in Gandhinagar, Gujarat. Himalayan Journal of Medicine and Surgery. 2025 Jan;6(1):1-5.
Download PDF
Review Article
Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review
Dharam Pau,
Tushar
Published: 05/04/2025
Download PDF
Cite
x
APA
Pau, D. & None, T. (2025). Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review. Himalayan Journal of Medicine and Surgery, 6(1), 1-3.
MLA
Pau, Dharam and Tushar . "Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review." Himalayan Journal of Medicine and Surgery 6.1 (2025): 1-3.
Chicago
Pau, Dharam and Tushar . "Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review." Himalayan Journal of Medicine and Surgery 6, no. 1 (2025): 1-3.
Harvard
Pau, D. and None, T. (2025) 'Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review' Himalayan Journal of Medicine and Surgery 6(1), pp. 1-3.
Vancouver
Pau D, Tushar T. Clinicopathological Profile of Colorectal Cancer Patients: A Contemporary Review. Himalayan Journal of Medicine and Surgery. 2025 Jan;6(1):1-3.
Download PDF
Research Article
Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra
Shallabh Sharma,
Ashish Guleria
Published: 05/04/2025
Download PDF
Cite
x
APA
Sharma, S. & Guleria, A. (2024). Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra. Himalayan Journal of Medicine and Surgery, 5(1), 1-5.
MLA
Sharma, Shallabh and Ashish Guleria. "Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-5.
Chicago
Sharma, Shallabh and Ashish Guleria. "Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-5.
Harvard
Sharma, S. and Guleria, A. (2024) 'Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-5.
Vancouver
Sharma S, Guleria A. Hernia and Its Surgical Management: A Cross-Sectional Study on Awareness Among the General Public of Kangra. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-5.
Sehgal, M. & Thakur, N. (2021). Evaluation of Effect of Various Co-Morbidities on Abdominal Wound Dehiscence after Midline Laparotomy in A Tertiary Care Hospital. Himalayan Journal of Medicine and Surgery, 2(2), 1-6.
MLA
Sehgal, Manjit and Naveen Thakur. "Evaluation of Effect of Various Co-Morbidities on Abdominal Wound Dehiscence after Midline Laparotomy in A Tertiary Care Hospital." Himalayan Journal of Medicine and Surgery 2.2 (2021): 1-6.
Chicago
Sehgal, Manjit and Naveen Thakur. "Evaluation of Effect of Various Co-Morbidities on Abdominal Wound Dehiscence after Midline Laparotomy in A Tertiary Care Hospital." Himalayan Journal of Medicine and Surgery 2, no. 2 (2021): 1-6.
Harvard
Sehgal, M. and Thakur, N. (2021) 'Evaluation of Effect of Various Co-Morbidities on Abdominal Wound Dehiscence after Midline Laparotomy in A Tertiary Care Hospital' Himalayan Journal of Medicine and Surgery 2(2), pp. 1-6.
Vancouver
Sehgal M, Thakur N. Evaluation of Effect of Various Co-Morbidities on Abdominal Wound Dehiscence after Midline Laparotomy in A Tertiary Care Hospital. Himalayan Journal of Medicine and Surgery. 2021 Jul;2(2):1-6.