Methods and Protocol
This narrative review was conducted from June 2021 to August 2021. Various databases such as PubMed/Medline, Google scholar, web of science, Scopus were searched to retrieve all possible studies to validate our point of interest. After searching the Mesh words of Almitrine, Inhaled Nitric Oxide (INO), ARDS, COVID-19, we extracted 20 articles in total, out of which we selected 16 full-text articles to be included in our study. All the patients Studied in the selected articles were COVID positive on PCR. They were on ventilatory support and completely sedated and relaxed with neuromuscular blocking agents to keep the patients on volume-control ventilation with target tidal volume (VT exp) of 6-7mL/hr according to predicted body weight (PBW) and PEEP for plateau pressure ≤30 cmH2O. Similarly, patients' arterial blood gases were analyzed at regular intervals of 2-4 hours and pH, PCO2, PO2, HCO3 and SAO2 levels were evaluated with a PCO2 target of less than 50 mmHg. The role of patient positioning was also of paramount significance, with the prone position being most effective in reducing oxygen requirement and ventilatory support with maintained blood oxygen saturation levels. In the same vein, soon after putting the patients from prone to supine a dose of 10ppm of INO alone followed by a combination of INO (10ppm) and 4, 8 and 10mcg/ml/min of Almitrine was administered and outcome parameters were tested.
Outcome Parameters of Given Therapy
Before the initiation of rescue therapy, the baseline parameters were assessed in terms of arterial blood gas analysis (pH, pCo2, pO2, HCO3 and Spo2), arterial partial pressure of oxygen/fraction of inspired oxygen (PaO2/FiO2), echocardiographic parameters like VTI LVOT (cm), Cardiac index (L/min/m2), TR velocity peak (m/s), LV eccentricity index and finally RV/LV surface ratio were also assessed before and after rescue therapy. Following the therapy administration, as mentioned above, the outcome measures were evaluated in supine baseline position, with alone INO and with both INO and Almitrine. Similarly, arterial blood gases were measured in supine baseline, INO alone and INO and Almitrine combined. Because of the effects of Almitrine on right ventricular afterload, echocardiography was also performed to assess any negative impact on the heart in terms of the following parameters (velocity–time integral of the left ventricular outflow tract, cardiac index). Finally, the effectiveness of the given therapy was assessed in terms of the paO2/Fio2 ratio. The increase in paO2/Fio2 ratio of 20% or 20mmHg was considered the actual response to the above-given therapy as observed in a study [7].
Mechanism Of Covid-19 Induced Ards
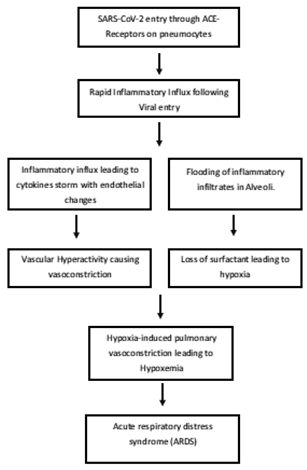
Coronavirus 2019, also known as SARS-CoV-2, entered the host through respiratory droplets and the host cells through ACE-2 receptors expressed on pneumocytes [8]. Soon after entry into the endothelial cells, the host response is activated, leading to a rapid influx of inflammatory cells and activation of various cytokines leading to cytokine storm. Accumulation of various cytokines and inflammatory infiltrates causes alteration in endothelial lining leading to endotheliitis and vascular Hyperactivity [9]. Under the influence of the inflammation, the flooding of alveoli with inflammatory infiltrates occurs, which ultimately causes loss of surfactant with intrapulmonary shunting of blood and hypoxemic alveoli. In response to alveolar hypoxia, hypoxia-induced pulmonary vasoconstriction occurs, leading to ARDS [10]. The Flow diagram of COVID-19 induced ARDS is given in Figure 1.
Baseline Parameters Befor e Initiation of Rescue Therapy
According to a study by Laghlam et al., the baseline means the value of PaO2/FiO2 in patients without rescue therapy was 146±48. Similarly, the mean value of partial pressure of CO2 in arterial blood without therapy was 52±8.9 [11]. In the same fashion, a study by François Bagate et al. has also reported the baseline characteristics in terms of pH = 7.30, PaCO2 = 48 mmHg, PaO2 = 102 mmHg, bicarbonate = 28 mmol/L and So2 = 97% in patients arterial blood analysis before initiation of rescue therapy. The baseline value of PaO2/FiO2 was about 77 without given therapy. Other observed parameters were also discussed as the echocardiographic findings with the velocity-time integral of left ventricular outflow tract (VTI LVOT) was 17cm, Cardiac index = 3.2 L/min/m2, Tricuspid regurgitation (TR) peak velocity = 2.8 m/s, Left Ventricular (LV) eccentricity index = 0.95 and finally, RV/LV surface ratio was observed that comes out to be 0.5 without rescue therapy [12].
Role of Inhaled Nitric Oxide (INO) Alone in Covid-19 Induced ARDS
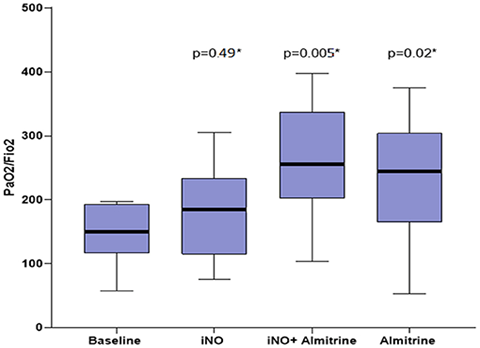
The role of Inhaled Nitric Oxide (INO) has been well documented since 1993 when it was first introduced as a wonder drug in reducing ventilatory requirements and improving arterial oxygen saturation in patients of ARDS [13]. It helps improve arterial oxygen concentration by its vasodilator activity and reducing hypoxia-induced pulmonary vasoconstriction through cGMP-dependent protein kinase pathway, thus improving ventilatory-perfusion (V/Q) mismatch [14]. The effectiveness of INO is validated by a study conducted by Laghlam et al., in which the authors have demonstrated the effects of INO in improving PaO2/FiO2 (mmHg) ratio from baseline value of 146±48 mmHg to 185±73 mmHg following INO as shown in Figure 2 [11]. Similarly, the arterial blood gas profile also showed marked improvement following INO administration where pH = 7.32, pCo2 = 45, pO2 = 124, bicarbonate = 26, SpO2 = 98% compared to baseline by a study from François Bagate et al. [12]. In the same vein, the echocardiographic findings were as follows: velocity-time integral of left ventricular outflow tract (VTI LVOT) = 16cm, Cardiac index = 2.8 L/min/m2, Tricuspid Regurgitation (TR) peak velocity = 2.2 m/s, Left Ventricular (LV) eccentricity index = 0.97 and finally RV/LV surface ratio was observed that comes out to be 0.44 with INO therapy [12].
Role Of Almitrine (DUXIL) Alone in Covid-19 Induced ARDS
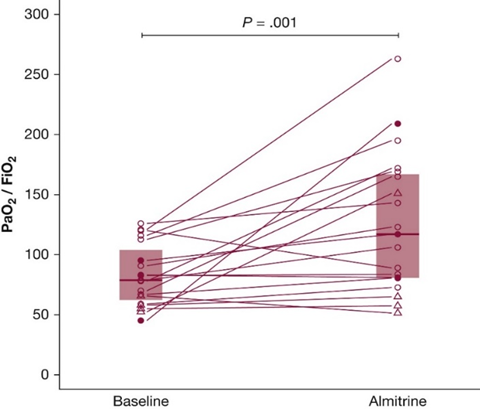
Almitrine (DUXIL) is an agonist on peripheral chemoreceptors expressed on carotid bodies and helps to improve ventilation in hypoxemic patients [2]. In the same vein, Almitrine also helps improve VA/Q mismatch by potentiating HPV at its lowest dose [15]. Various studies have tested the different doses of Almitrine (8 µg/kg/min, 4 µg/kg/min and 10 µg/kg/min) to elaborate the dose-dependent effects of Almitrine; to surprise all the administered doses were showing significant responses in terms of rising in PaO2/FiO2 (mmHg) ratio from baseline values [11,12,16]. Similarly, a study by Romain Barthélémy et al. on the effectiveness of Almitrine in improving the PaO2/FiO2 (mmHg) ratio was showing a significant rise in this ratio from the baseline value of 79 mmHg to 117 mmHg following administration of low dose (2 µg/kg/min) of Almitrine as shown in Figure 1 [17]. The effectiveness of Almitrine is also validated by a study conducted by Laghlam D et al., in which the authors have demonstrated the effects of Almitrine in improving the PaO2/FiO2 (mmHg) ratio from the baseline value of 146±48 mmHg to 238±98 at the dose of 8 µg/kg/min [11]. According to blood gas analysis the baseline values of were pH = 7.38, PaCO2 = 42, paO2 = 135, bicarbonate = 25.1 and central venous O2 saturation was 73%, similarly following the administration of Almitrine (12 µg/kg/min) the blood gas profile improved pH = 7.41, PaCO2 = 43, PaO2 = 215, bicarbonate = 24.8 and central venous oxygen saturation of 85 as compared to baseline values [18]. Similarly, on 2D Transesophageal Echocardiographic (TEE), findings showed improvement of the cardiac index from the baseline value of 2.6 to 3.0 l/min–1/m–2 following 12hrs after Almitrine infusion [16]. The effectiveness of Almitrine alone is represented in Figure 2.
Role of INO and Almitrine Combined in COVID-19 Induced ARDS
The therapeutic effectiveness of both INO and Almitrine combined has been validated by recent studies in patients with COVID-19 induced ARDS. Studies have also depicted the significant role of combined INO and Almitrine in improving patients' PaO2/FiO2 (mmHg) ratio and blood gas profile compared to baseline, INO alone and Almitrine alone. A study by Laghlam D et al. had reported the significant rise in PaO2/FiO2 (mmHg) ratio from the baseline value of 146±48 mmHg to 255±90 followed by INO and Almitrine combination when INO was continuously given at the dose of 10 ppm through the inspiratory limb of the ventilator. Similarly, Almitrine was delivered intravenously via a central venous catheter at a concentration of 8 µg/kg/min, as shown in Figure 2 [11]. In the same vein, the arterial blood gas analysis reports as reported by François Bagate et al. are also depicting the significant improvement in blood gas analysis profile from baseline values of pH = 7.30, PaCO2 = 48 mmHg, PaO2 = 102 mmHg, bicarbonate = 28 mmol/L and So2 = 97% to pH = 7.32, PaCO2 = 46 mmHg, PaO2 = 180 mmHg, bicarbonate = 28 mmol/L and So2 = 99% after the combined dose of INO and Almitrine [12]. The echocardiographic parameters were also noted and they were as follows: velocity-time integral of left ventricular outflow tract (VTI LVOT) = 20cm, Cardiac index = 2.9 L/min/m2, Tricuspid Regurgitation (TR) peak velocity = 2.7 m/s, Left Ventricular (LV) eccentricity index = 0.97 and finally RV/LV surface ratio was observed that comes out to be 0.49 with both INO and Almitrine therapy [12]. The effectiveness of both Almitrine and INO is represented in Figure 3.