Management of Neonatal Occlusions in the Surgery Department of the Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori in Libreville from January 1, 2019 to December 31, 2021
Mélina Nkole Aboughe
1
,
J. H. Nzue Nguema
1
,
E. Comlan
2
,
S. Ipouka
1
,
F. Ondo Ndong
3
1
Department of Pediatric Surgery Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori, Gabon
2
Centre Hospitalier Universitaire de Libreville Surgery Department, Gabon
3
Centre Hospitalier Universitaire, Mère-Enfant Fondation Jeanne Ebori Resuscitation Service, Gabon
Introduction: Neonatal intestinal obstruction is an occlusive syndrome marked by a delay or absence of intestinal transit most often due to an obstacle downstream of the pylorus. It is the consequence of a functional and/or mechanical anomaly. This is a frequent medical and surgical emergency in neonatology. The difficulty of its management as well as the lack of data on the issue in our country led us to study the different therapeutic methods and their results. Objective: To study the therapeutic methods and the results of the management of neonatal intestinal occlusions in the surgery department of the Mother-Child Foundation Jeanne Ebori University Hospital. Patients and Methods: This is a descriptive and retrospective study from January 1, 2019 to December 31, 2021. It focused on all newborns from 0 to 28 days old presenting with an occlusive syndrome or having presented it during hospitalization, during our study period. Results: Over this period, 69 newborns presented neonatal intestinal obstruction, i.e. a frequency of 25.2% of surgical emergencies operated on during that period. Ulcerative-necrotizing enterocolitis and ano-rectal malformations were the most seen. Treatment was based on etiology. The mortality rate was 32%. Conclusion: ONN are frequent and burdened with high mortality in our country. they are dominated by anorectal malformations and ulcerative-necrotizing enterocolitis. The improvement of diagnostic and therapeutic delays, the optimization of antenatal diagnosis and the awareness of midwives, gynecologists and pediatricians on these different conditions would improve their prognosis.
Keywords
Intestinal Obstruction
Newborns
Care
Libreville
INTRODUCTION
Neonatal Intestinal Obstruction (NNO) is an occlusive syndrome marked either by a delay or by the absence of intestinal transit, most often due to an obstacle downstream of the pylorus [1]. It is the consequence of a functional and/or mechanical anomaly. It is a frequent medico-surgical emergency in neonatology [2]. It ranks second among surgical pathologies after wall pathologies [2].Its frequency is different depending on the country. In Niger, Ali and coll [3] reported a frequency of 31.9%, in Nigeria Ademuyiwa and coll [4] found 23.5%. In Morocco Imane O and coll found a frequency of 25.5% in 2017 [5].The diagnosis of NNO is based on clinical and paraclinical examinations. It can be evoked in the antenatal period during the ultrasound of the 2nd and 3rd trimester in front of a polyhydramnios, a dilation of the digestive loops and the hyperchogenicity of the hail [1].Whatever the etiology, mortality in developing countries varies from 20 to 70%; this high mortality is linked to the diagnostic and therapeutic delay which varies from one series to another. In Mali a mortality of 32% in 2008 was found by Aliou T and coll [1] and in Morocco, it was 39% according to Imane and coll in 2017 [5].Mortality is low in developed countries where the diagnosis is most often antenatal, allowing early medical and surgical treatment [6,7].In sub-Saharan Africa, particularly in GABON, the diagnostic and therapeutic problems of these conditions remain. The lack of data on the issue led us to carry out this study, the main purpose of which is to contribute to improve the care of newborns with ONN.
MATERIALS AND METHODS
Type and Duration of the StudyThis is a descriptive and retrospective study which took place over a period from January 1, 2019 to December 31, 2021, i.e. over a period of 3 years.Study FrameworkThis study took place in the neonatal medicine and pediatric surgery departments of the Jeanne Ebori Foundation mother-child university hospital center (CHUME-FJE).
Study PopulationInclusion Criteria: We included in our study all newborns (0 to 28 days), admitted to the services for confirmed occlusive syndrome or having presented an occlusive syndrome during hospitalization during the study period.
Criteria for Non-InclusionEsophageal atresia and incomplete records were not included.Data CollectionThe data collection was made from the medical records of hospitalization of the neonatal medicine department of pediatric surgery and the registers of the operating room of the CHUMEFJE. These data were then collected on a standardized form.Statistical AnalysisStatistical analysis was performed with SPSS software version 24. Categorical variables were expressed as a percentage and quantitative variables as mean and standard deviation. The association between qualitative variables was assessed by the Chi2 test (or Fisher test for small numbers) and the comparison of means by the Mann Whitney/Wilcoxon test. The significance threshold was set at 5%.
RESULTS
FrequencyDuring the study period, 1140 patients were hospitalized in the pediatric surgery department of CHUME-FJE. Among which 661 operated. The patients operated for a surgical emergency numbered 274. Those who presented NNO were 74. Sixty-nine patients met the inclusion criteria.Thus the ONN represented a frequency of 6.05% of operated patients, 10% of hospitalized patients and 25.2% of operated emergencies.Sociodemographic DataSex: Forty-four patients were male (63.7%). The sex ratio was 1.9.
AgeThe average age was 5.4±6.3 days with extremes of 0 to 25 days. Fifty-five patients (79.7%) were less than 7 days old.
OriginFifty patients resided in urban areas (72.4%) and 27.5% in rural areas. In 87.0% of cases, patients came from a health facility, including 63.7% from university hospitals.
Clinical DataBackground: Forty-one patients (59.4%) had practiced at least 4 (prenatal consultation) CPN and twenty-eight (40.5%) more than 4 CPN.Fourteen patients had not performed an ultrasound in the 1st trimester of pregnancy and 11 in the 3rd trimester.Prenatal diagnosis was not made in any patient.In our series, 27 newborns were born prematurely (39%). Among them, 22 presented an average prematurity (81.5%), 5 severe premature newborn (18.5%).
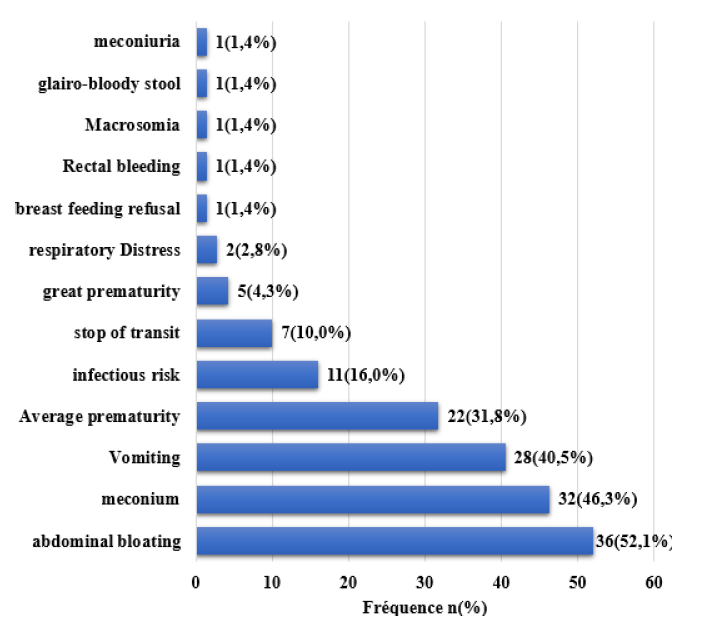
Reason for AdmissionFigure I provides information on the distribution of newborns according to the reasons for admission.Bloating was the reason for admission in 52.1% of cases, followed by meconium emission anomaly (46.3%) and vomiting in 40.5%.
Figure 1: Distribution of Newborns According to Reasons for Admission
Admission DeadlineThe average admission time was 2.2±1.7 days. It was ≤ 2 days in 62%.
Anthropometric ParametersIn our series, 27 newborns were born prematurely, a proportion of 39.0%. Among them, 22 presented an average prematurity and 5 a great prematurity.On admission, 48 newborns weighed between (2500-4000 g), 15 weighed between (1500-2500 g), 5 weighed less than 1500 g and 1 weighed more than 4000 g (Table 1).
Table 1: Anthropometric Data
Constants
Means and standard deviations
Extrêmes
Size (cm)
46,5±5,3
31-53
Intake weight (g)
2696,5±804
600-5000
Clinical SignsFunctional Signs: The delay or absence of meconium emission was observed in 32 patients or 46.3% (Table 2).
Table 2: Distribution of Patients According to Functional Signs
Functional signs
n
%
Delay/absence of meconium emission
32
46,3
Vomiting
Bilious
18
26
Food
9
13
Fécaloid
1
14
Stop of materials
7
10
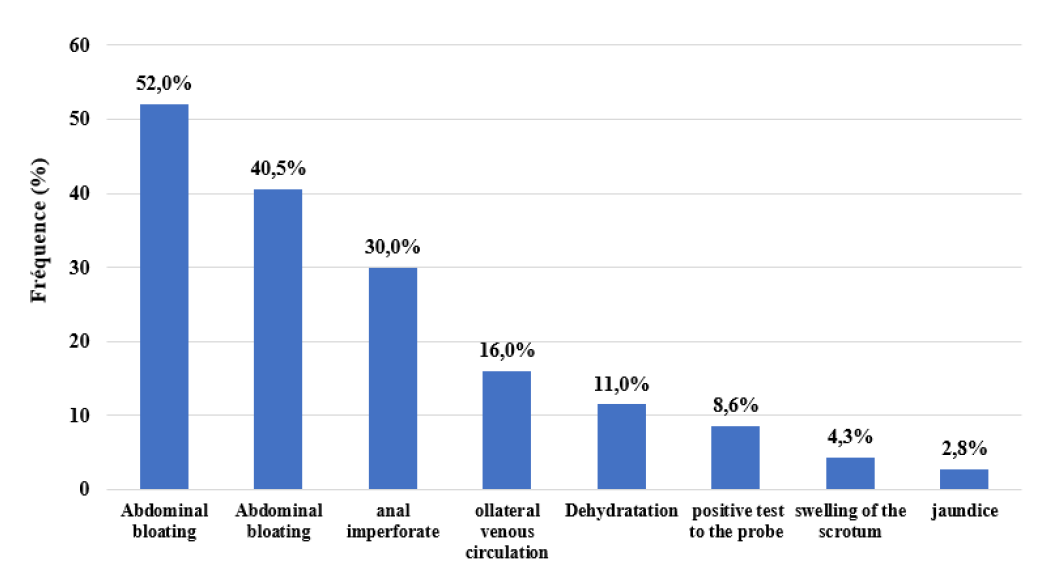
The physical examination found abdominal distension in 36 patients, i.e. 52% (Figure 2).
Figure 2: Distribution of Patients According to Physical Signs
Paraclinical DataBiological Data: Natremia was lowered in 31.0% of patients with an average of 131.55±10.76 mmol/L.CRP was high in 50.7% of patients with an average of 60.85±83.47 mg/L >15 mg/L and extremes of 1 to 390 mg/L.NFS was performed in all patients. The average hemoglobin level was 13.6 g/dl with extremes of 6.7 and 20.8 g/dl, 53.7% newborns had anemia. The average leukocyte rate was 10664 elements/ml with extremes of 1050 and 37770 elements/m, 24.6% presented with leukopenia and 26% with hyperleukocytosis. The mean platelet count was 333,458 elements/ml with extremes of 36,000 and 644,000 elements/ml, 37.6% had thrombocytopenia and 10 thrombocytosis.
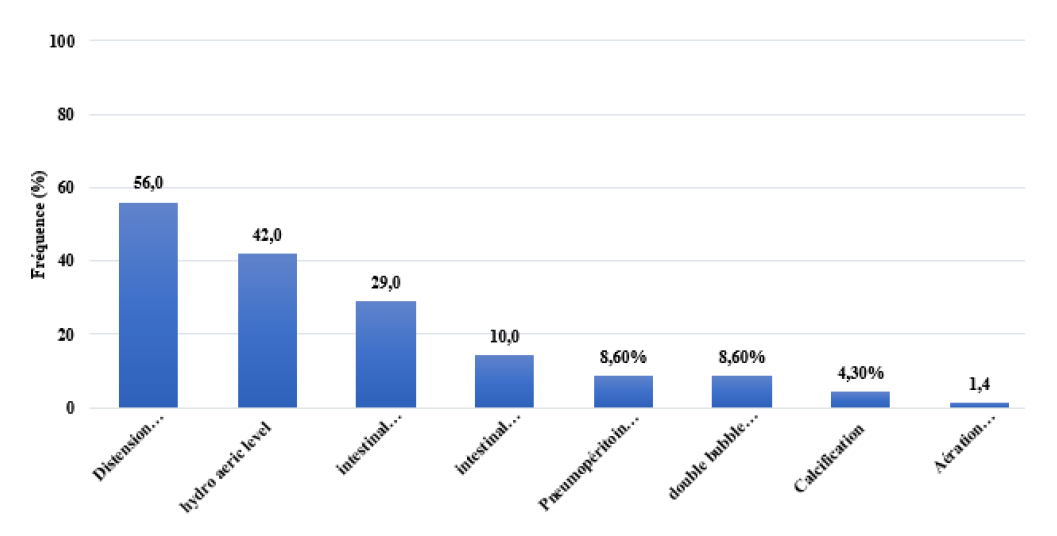
Morphological DataAbdomen Without Preparation (AWP): Figure 3 shows the distribution of patients according to the results of the (AWP).
Figure 3: Distribution of Patients According to AWP Results
WAGENSTEEN and RICE IncidenceIt was performed in 16 newborns (23%) and found 10 cases of high anorectal malformation (ARM, 63%), 1 case of intermediate ARM (6%) and 5 cases of low ARM (31%).
UltrasoundAbdominal ultrasound was performed in 18 patients. The results have been shown in the table. Digestive aerocoly was the most observed ultrasound sign in 27.7% of cases.
Other ExamsTwo newborns had performed a esogastroduodenal transit in favor of duodeno-jejunal dilation, 2 water-soluble enemas in favor of a microcolon appearance and a CT scan in favor of pneumoperitoneum with peritoneal effusion were performed.
Time To DiagnosisThe average diagnostic delay was 3.12±2.36 days with extremes of 1 and 13 days.
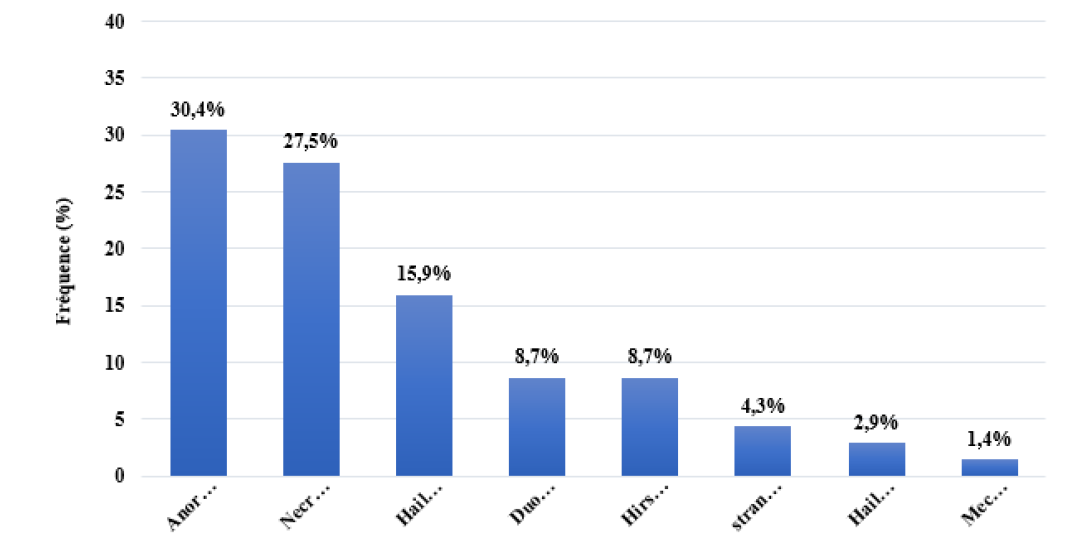
Etiological DataIn our study ARM represented 30% of etiologies among them, high forms in 15 cases (71.4%), intermediate in 1 case (4.7%) and low forms in 5 cases (23.8). Associated malformations were found in 7 cases (33.3%) including 3 cases of urogenital malformations, 2 esophageal atresia, 1 case of dextrocardia, 1 case of trisomy 21 (Figure 4).
Figure 4: Distribution of Patients According to Etiology
Therapeutic DataMedical Treatment: Pre, per and post operative resuscitation was performed in all patients and included:
A correction of hydro-electrolyte disorders
The placement of a nasogastric tube,
Administration of a broad-spectrum antibiotic therapy (Betalactamine+Aminoside+Imidazole, Betalactam+Aminoside+Imidazole)
Parenteral nutrition made of infusion solution
Surgical TreatmentIn our series, 44 patients underwent surgery. The three main surgical procedures performed were colostomy in 34.1% of cases, end-to-end resection anastomosis in 31.8% of cases and duodeno-duodenostomy in 13.6% of cases.
Surgical Intervention TimeThe average time elapsed between the date of admission and the date of surgery was 3.38±1.14 days for all operated with extremes of 1 and 21.The mean time between symptoms and intervention was 4.25±2.20 days with extremes ranging from 1 to 25 days (Table 3).
Table 3: Distribution of Patients According to the Surgical Procedure Performed
Surgical procedure
n (%)
Etiology (n)
Colostomy
15 (34,1)
Anorectal malformation (14)
Hirschsprung disease (1)
End-to-end resection anastomosis
14 (31,8)
Hail atresia (11)
Necrotizing ulcerative enterocolitis (2)
Hail Volvulus (1)
Duodéno-duodénostomy
6 (13,6)
Duodénale atresia (6)
Anorectoplasty
5 (11,4)
Anorectal malformation (5)
Hernia repair
3 (6,8)
Strangulated inguino scrotal hernia (3)
Hail detorsion
1 (2,3)
Hail Volvulus (1)
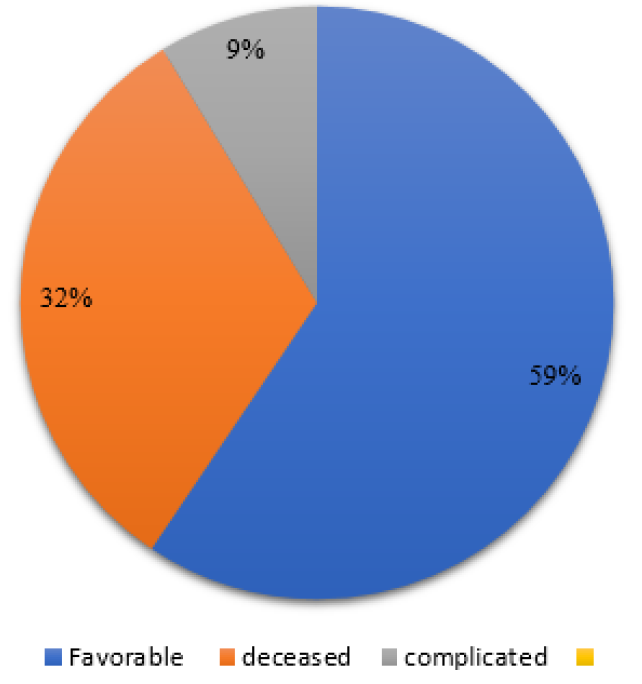
EvolutionComplications were noted in 9% (n = 6) patients and then resolved. These were: jaundice (in 2 cases), severe anemia (2 cases), malnutrition (in 1 case) and dehydration (in 1 case) (Figure 5).
Figure 5: Distribution of Patients According to the Evolution
Mortality RateIn our series, 22 (31.8%) patients had died (9 non-operated patients and 13 operated patients).
Operative MortalityOf the 44 patients operated on, 13 patients died, 2 intraoperatively and 11 postoperatively. The circumstances of death were 10 cases of septic shock, 3 cases of severe malnutrition.
Characteristics of Deceased PatientsPatient Mortality by Etiology: In our study, 7 deceased patients had ECUN, i.e. 31.8%.5 ARM (22.7%), 4 (18%) duodenal atresia, 3 (13.6%) small bowel atresia, 2 volvulus on common mesentery, 1 Hirschsprung disease.Among the 22 patients who died, 16 were male, 9 were premature 16 were less than 7 days old (Table 4).
Table 4: Provides Information on the Characteristics of Deceased Patients
Parameterss
n
Sex
M
16
F
6
Age at intake
≤7
16
≥14
6
Weight
≤2500
8
2500-4000
14
≥4000
0
AGE
<37
13
≥37
9
Surgery
Yes
15
No
7
DISCUSSION
The general objective of this work was to study the therapeutic methods and the evolution of neonatal occlusions at the CHUME FJE. Our study has a limitation due to its retrospective nature.
Frequency
NNO represented a frequency of 6.05% of operated patients, 10% of patients hospitalized in surgery, 1.7% of neonatal medicine hospitalizations and 25.2% of operated emergencies. In Bamako Kone [4] found that NNO represented 0.7% of hospital frequency, 3.92% of all operated cases and 8% of surgical emergencies. It must be said that the population studied was much larger than ours (1301/13122 cases). There are factors predisposing to the occurrence of congenital malformations, in particular cultural practices such as consanguineous marriages [8-10].
Sociodemographic DataHistory and Comorbidities:
In our series. Three quarters of the patients had performed a maximum of 4 CPNs, according to the WHO [11], it is recommended to perform 8 CPNs. This therefore amounts to saying that more than three quarters of women had poorly followed pregnancies. not allowing early detection of anomalies. In our countries, it is very often during an occlusive episode that the diagnosis is made. [12,13], rather than following an antenatal ultrasound.In our series, 27 newborns were born prematurely (39%). According to Moukiti and coll [14] prematurity is the most important predictor of (necrotisis ulcerative enterocolitis ) ECUN.
Age
The average age of our series was 5.4±6.3 days with extremes of 0 to 25 days. They are comparable to those found in Mbonicura JC and coll [15] with an average age of 6.8 ±5.1 days with extremes of 1 and 24 days. Indeed these similarities could be explained by the delimitation of the age group which was between 0-25 days. These results are lower than those found by Hounnou GM and coll [16] where the average age at admission was 14 days±5 with extremes at 1 and 55 days. Our average age which is low compared to that found by Hounnou GM and coll [16] could find its explanation in the definition of the limits of the neonatal period in our respective studies. Indeed, the neonatal period in our study was defined as that ranging from 0 to 28 days unlike the other author who considered it as a period ranging from 0 to 55 days. According to the WHO, this period is from birth to 28 days of age.
Sex
The predominance was male with a sex ratio of 1.9. This predominance was found by Saleem and coll [17]. Gender is not a factor in the occurrence of neonatal intestinal obstruction [18]. The male predominance observed in our study is consistent with data from the literature.
Weight
The average weight at admission was 2695±80 g with extremes of 600-5000. These results are similar to those found by Hounnou and coll [16] who found an average weight of 2648±152 g with extremes of 1430 g and 3530 g, Mbonicura and coll [15] who found 2844±152 g with extremes 2000-4000g. weight is not incriminated as a risk factor for occurrence but can influence prognosis [16]. Nagpure and coll [19] demonstrated in their study that newborns weighing less than 2000 g had a high mortality rate of 81.6% against 1.3% mortality in newborns weighing more than 2000g. Prematurity and hypotrophy have been described by some authors as being risk factors for ECUN [20,21].
Clinical Data
Etiological diagnosis, treatment and evolution.
Admission Deadline
Mbonicura and coll [15] who found an average delay of 3.51±2.88 days. This delay is lower than those found by Ali and coll [3] who found an average delay of 4.7 days and Hounnou and coll [16] with an average delay of 11±4 days. Our delay remains quite long for a pathology with rapid evolution potential.In our developing countries, it is in front of the occlusive picture in a newborn that the diagnosis is made. Unlike in developed countries where the diagnosis is most often antenatal, allowing early medical and surgical management [15,16]. In most developed countries, early diagnosis, including prenatal diagnosis and planned delivery in a fully equipped pediatric surgical center, has significantly improved newborn survival [22].In addition, the lack of knowledge of these conditions by certain medical or paramedical practitioners who refer newborns late, sometimes consulted quite early [ 23].
Reason for Hospitalization
The 3 main reasons for hospitalization observed in our study were abdominal distension (52.1%), abnormal emission of meconium (46.3%) and vomiting (40.5%). These results are similar to different proportions to those of Ali et al. [3] and Imane et al. [5].
Etiologies and Their Treatment
The most common etiologies were: ARM (30%), enterocolitis (27%) and small bowel atresia (16%).This agrees with data from the teams of Rehman [24], Ada [25] Inyang [26 ], Talari [27]. There were 17 newborn males and 4 females, their age varied between 1 and 15 days. Mean time to admission was 3.35±2.52 days. The clinical examination in our series found: 23 cases of abdominal bloating (33.3%), 23 cases of abnormal emission of meconium (33.3%). Kassanga and coll [28] had mainly found the occlusive syndrome in 50% followed by meconiuria and anal imperforation.The management consisted in: fourteen colostomies (13 high ARM and 1 intermediate ARM), 05 (low ARM) benefited from anorectoplasty. Kasanga [28] and Habou [29] recommend colostomy in high and intermediate forms and anorectoplasty in low forms. The death rate of MAR was 22.7% (n = 3/19). These were three patients who could not be operated on because they died before surgery. Kasanga and coll [28] found 25% and Habou and coll [29] 17%.
Ulcerative Necrotizing Enterocolitis (ECUN)
Nineteen cases of ulcerative-necrotizing enterocolitis were collected in our study, i.e. 27.5% of cases Uchenna E and coll [30] in Nigeria found 48.8% and Nandi B and coll [31] in Canada found found 72%. The results vary from country to country. Prematurity and low weight have been recognized as the 2 most consistent risk factors for ECUN [20,21].Indeed, abdominal distension, infectious syndrome and vomiting on the ground of prematurity were revealing signs of ECUN in newborns, especially before confirmation using radiology. The thoraco-abdominal X-ray was performed in all newborns, it was found mainly intestinal pneumatosis (pathognomonic sign of ECUN) in 89% of cases. This predominance was found in Moukity and coll [14] who found pneumatosis intestinalis in 71.4% of cases.Urgent medical treatment was based on rehydration, fasting, placement of a nasogastric tube, correction of electrolyte disorders and antibiotic therapy, the most used combination of which was 3rd generation cephalosporin + imidazole + Aminoside. Of the 19 patients, seven died, five of whom had received strictly medical treatment and two surgical treatment. Moukity and coll only medical treatment had been undertaken. In the Phani [32] and Cassir [33] teams, surgery was necessary in 50% of cases. The ECUN mortality rate was 36%. Moukity and coll found a mortality of 49%. The death rate from enterocolitis is still high in our country.
Small Bowel Atresia
We identified 11 cases (16%) of small bowel atresia, 1%. It is lower than that found in Hounnou [16].Their age varied between 2 and 25 days. All parturients had performed a 2nd-3rd trimester ultrasound and no abnormality had been detected. Unlike Awana et al. [35], Kasanga [34] Calisti et al. [28] in whom ultrasound revealed polyhydramnios suggesting a digestive anomaly. All patients underwent end-to-end resection anastomosis. According to the literature, it is the most commonly used surgical treatment [23,36]. The postoperative course was favorable in 9 patients, 3 patients had died, i.e. a mortality of 4.3%. (2 septic shocks, severe malnutrition), Maonea and coll had found a mortality of 100% the circumstance of death was severe dehydration.
Hirschsprung Disease
It represented 8.6% of etiologies in our study. This result is similar to that of Talari et al. [37] who found 9.3%. It concerned 5 newborns males and 1 female. The average age of admission was 2.66±6.38 days. For Sekou and coll [38] the average age was 42 months. This age difference could be explained by the fact that in our sample the age ranges were 0-28 days while Sekou had a sample with age ranges of 0-16 years.The clinical examination mainly found: meconium emission abnormality, abdominal bloating, positive probe test, enterocolitis and vomiting and a similarity had been found by some authors [38].In our series, all the patients had benefited from nursing and 1 patient was complicated by enterocolitis and had benefited from a colostomy. Sékou and coll [38], performed nursing in 66 (73%) of cases and a colostomy in 25 (27%). Bandre and coll [39], had practiced nursing in 67.3% and a colostomy in 75%. Our results agree with data from the literature [38,40]. The mortality was 1.4%. This result is comparable to other authors [38,40].
CONCLUSION
At the end of our study on the management of neonatal occlusions in the surgery department of the mother-child university hospital of Libreville from 2019 to 2021, we can say that neonatal occlusions are frequent conditions, burdened with high mortality. They represent 10% of the department's surgical activity and a quarter of the emergencies operated on. The most frequently encountered etiologies are anorectal malformations (30.4%), ulcerative necrotizing enterocolitis (27.5%) and small bowel atresia (16%). Their management was mainly surgical (63.7%) but also medical (36.2%). Unfortunately 31.9% of them died.The improvement of diagnostic and therapeutic delays, the optimization of antenatal diagnosis and the awareness of midwives, gynecologists and pediatricians on these different conditions would improve their prognosis. Finally, collaboration between neonatologists, gynecologists, resuscitators and pediatric surgeons would be a major asset in reducing the lethality of these pathologies.
REFERENCES
Ma, B. et al. “Neonatal small bowel obstruction at sylvanus olympio teaching hospital of lomé.” Journal Africain de Chirurgie Digestive, vol. 14, no. 2, 2014, pp. 167–171.
Seth, A. and R. Chanchlani. “Neonatal gastrointestinal emergencies in a tertiary care center in Bhopal, India: A prospective study.” Journal de Chirurgie de l’USS, vol. 1, no. 5, 2020, pp. 1–8.
Ali, A. et al. “Occlusions intestinales néonatales: Aspects diagnostiques, thérapeutiques et évolutifs au service de chirurgie pédiatrique de l’hôpital national de lamordé de niamey.” Annales de l’Université Abdou Moumouni, vol. 2, no. 1, 2017, pp. 1–11.
Ademuyiwa, O. et al. “Determinants of mortality in neonatal intestinal obstruction in Ile-Ife, Nigeria.” African Journal of Pediatric Surgery, vol. 6, no. 1, 2009, pp. 11–13.
Imane, O. Les Occlusions Néo-natales. Doctoral thesis, Faculté de Médecine et Pharmacie de Marrakech, 2017.
Ali, I. et al. “Assessment of predictors of mortality in neonatal intestinal obstruction.” Journal of Neonatal Surgery, vol. 7, no. 1, 2018, pp. 1–6.
Nagpure, A. et al. “Etiological spectrum of neonates presenting with intestinal obstruction at a tertiary care centre.” Journal of Medical Science and Clinical Research, vol. 88, May 2016, pp. 10562–10567.
Kaboré, A. et al. “Les malformations congénitales: Étude descriptive hospitalière à ouagadougou.” Journal of Medical and Biomedical Sciences, vol. 21, no. 3, 2020, pp. 90–99.
Obu, H. et al. “Congenital malformations among newborns admitted in the neonatal unit of a tertiary hospital in enugu, south-east Nigeria.” BMC Research Notes, 2012, pp. 1–7.
Masood, S. “Congenital malformations in newborns of consanguineous and non-consanguineous parents.” Pakistan Journal of Medical Sciences, vol. 27, no. 1, 2011, pp. 1–6.
World Health Organization. Recommandations de l’OMS Concernant les Soins Prénatals pour que la Grossesse Soit une Expérience Positive. Organisation Panaméricaine de la Santé, 2018.
Ademuyiwa, A.O. et al. “Determinants of mortality in neonatal intestinal obstruction in Ile-Ife, Nigeria.” African Journal of Paediatric Surgery, vol. 6, no. 1, 2009, pp. 11–13.
Atarraf, K. et al. “L’Atrésie Colique : À propos de deux cas.” Pan African Medical Journal, vol. 7, no. 1, 2011, pp. 1–10.
Moukity Mbongo, E. Enterocolite Ulcéro-nécrosante du Nouveau-né à Libreville. Doctoral thesis, Université des Sciences de la Santé, 2021.
Mbonicura, J.C. et al. “Factors associated with mortality in neonatal intestinal obstructions at kamenge teaching hospital (burundi).” Aditum Journal of Clinical and Biomedical Research, 2021, pp. 4–7.
Hounnou, G.M. et al. “Les occlusions néonatales au centre national hospitalier et universitaire de cotonou.” Clinical Mother and Child Health, vol. 3, 2006, pp. 457–464.
Saleem, M. et al. “Jejunoileal atresia: A case series of 63 neonates and risk factors for mortality.” Annals of Pediatric Surgery, vol. 18, no. 12, 2022, pp. 1–5.
Carter, B.M. and D. Holditch-Davis. “Risk factors for NEC in preterm infants: how race, gender and health status contribute.” Advances in Neonatal Care, vol. 8, no. 5, 2008, pp. 285–290.
Nagpure, A. et al. “Etiological spectrum of neonates presenting with intestinal obstruction at a tertiary care centre.” Journal of Medical Science and Clinical Research, vol. 88, May 2016, pp. 10562–10567.
Nkole, A. et al. “Morbidity and mortality of surgical emergencies in premature newborns: About 34 cases.” Himalayan Journals, vol. 21, no. 4, 2021, pp. 1–2.
Chabernaud, J. and E. Giannoni. L’entérocolite nécrosante du prématuré. Doctoral thesis, Faculté des Sciences Pharmaceutiques et Biologiques de Lille, 2017.
Seth, A. et al. “Urgences gastro-intestinales néonatales dans un centre de soins tertiaire à bhopal, inde : une étude prospective.” Journal de Chirurgie de l’USS, vol. 1, no. 5, 2020.
Barak, B. “Les occlusions néonatales du grêle au CHU SO.” Journal Africain de Chirurgie Digestive, vol. 14, no. 2, 2019.
Rehman, S.U. et al. “Pattern and outcome of neonatal gastrointestinal surgical emergencies: A prospective analysis.” Professional Medical Journal, vol. 28, no. 3, 2021, pp. 415–421.
Ada, A. et al. “Les pathologies chirurgicales néonatales à l’hôpital national de lamordé de niamey.” European Scientific Journal, vol. 13, no. 24, 2017, pp. 156–164.
Inyang, A. “Étude rétrospective de l’occlusion intestinale néonatale à calabar: Étiologie et évolution.” Nigerian Journal of Paediatrics, vol. 41, no. 2, 2014, pp. 96–98.
Talari, V.K. and S. Kumar Sipala. “Une étude clinique de l’obstruction intestinale néonatale.” Journal of Dental and Medical Sciences, vol. 16, August 2017, pp. 8–14.
Kasanga, T.K. et al. “Malformations anorectales: Revue de six ans aux cliniques universitaires de lubumbashi.” Pan African Medical Journal, vol. 38, 2021, pp. 9.
Habou, O. et al. “Les malformations anorectales dans le service de chirurgie pédiatrique de l’hôpital national lamordé de niamey.” Annales de l’Université Abdou Moumouni, June 2015, pp. 71.
Uchenna, E. et al. “Obstruction intestinale néonatale: Une expérience de cinq ans dans un hôpital tertiaire d’enugu, Nigéria.” Journal de Chirurgie (Paris), vol. 7, no. 5, 2019, pp. 138–142.
Nandi, B. et al. “A comparison of neonatal surgical admissions between two linked surgical departments in Africa and Europe.” Pediatric Surgery International, vol. 24, no. 8, 2008, pp. 939–942.
Phani Kiran et al. “Necrotizing enterocolitis: Current perspectives.” Dove Press Journal, 2014, pp. 31–42.
Cassir, N. et al. “Clostridium butyricum strains and dysbiosis linked to necrotizing enterocolitis in preterm neonates.” Clinical Infectious Diseases, vol. 61, 2015, pp. 1107–1115.
Calisti, A. et al. “Jejunoileal atresia: Factors affecting the outcome and long-term sequelae.” Journal of Clinical Neonatology, vol. 1, no. 1, 2012, pp. 4–4.
Awana, P.A. et al. “Antenatal sonographic diagnosis of jejunal atresia presenting as secondary hydramnios.” Journal of Medical and Biomedical Sciences, vol. 22, no. 7, 2021, pp. 119–120.
Maoneo, A. et al. “Atrésie du Jéjuno-iléon: À propos d’un cas.” 2015, pp. 138–141.
Talari, V.K. and S. Kumar Sipala. “Une étude clinique de l’obstruction intestinale néonatale.” Journal of Dental and Medical Sciences, vol. 16, August 2017, pp. 8–14.
Sekou, D. Maladie de Hirschsprung: Aspects Épidémiologiques, Cliniques, Thérapeutiques et Évolutifs. Doctoral thesis, Université des Sciences, des Techniques et des Technologies de Bamako, 2021.
Bandré, E. et al. “Hirschsprung’s disease: Management problem in a developing country.” African Journal of Paediatric Surgery, vol. 7, no. 3, 2010, pp. 166–168.
Anderson, J.E. et al. “Epidemiology of hirschsprung disease in california from 1995 to 2013.” Pediatric Surgery International, vol. 34, no. 12, 2018, pp. 1299–1303.
License
Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
All papers should be submitted electronically. All submitted manuscripts must be original work that is not under submission at another journal or under consideration for publication in another form, such as a monograph or chapter of a book. Authors of submitted papers are obligated not to submit their paper for publication elsewhere until an editorial decision is rendered on their submission. Further, authors of accepted papers are prohibited from publishing the results in other publications that appear before the paper is published in the Journal unless they receive approval for doing so from the Editor-In-Chief.
Himalayan Journal of Medicine and Surgery open access articles are licensed under a Creative Commons Attribution-Share A like 4.0 International License. This license lets the audience to give appropriate credit, provide a link to the license, and indicate if changes were made and if they remix, transform, or build upon the material, they must distribute contributions under the same license as the original.
Advertisement
Recommended Articles
Research Article
Effect of Land Degradation on Livelihood
Kemalo Abdulmalik,
Isreal Zewide
Published: 04/01/2024
Download PDF
Cite
x
APA
Abdulmalik, K. & Zewide, I. (2024). Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery, 5(1), 1-4.
MLA
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5.1 (2024): 1-4.
Chicago
Abdulmalik, Kemalo and Isreal Zewide. "Effect of Land Degradation on Livelihood." Himalayan Journal of Medicine and Surgery 5, no. 1 (2024): 1-4.
Harvard
Abdulmalik, K. and Zewide, I. (2024) 'Effect of Land Degradation on Livelihood' Himalayan Journal of Medicine and Surgery 5(1), pp. 1-4.
Vancouver
Abdulmalik K, Zewide I. Effect of Land Degradation on Livelihood. Himalayan Journal of Medicine and Surgery. 2024 Jan;5(1):1-4.
Download PDF
Research Article
Gastric Cancer: A Comprehensive Review
Ali Shafeeq Neameh,
...
Hussein Riyadh Ali Shlaka
Published: 20/01/2026
Download PDF
Cite
x
APA
Neameh, A. S., Hatab, W. M. & Ali Shlaka, H. R. (2026). Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery, 7(1), 1-5.
MLA
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-5.
Chicago
Neameh, Ali S., Waleed M. Hatab and Hussein R. Ali Shlaka. "Gastric Cancer: A Comprehensive Review." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-5.
Harvard
Neameh, A. S., Hatab, W. M. and Ali Shlaka, H. R. (2026) 'Gastric Cancer: A Comprehensive Review' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-5.
Vancouver
Neameh AS, Hatab WM, Ali Shlaka HR. Gastric Cancer: A Comprehensive Review. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-5.
Download PDF
Research Article
Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess
Asaad Mezher Hussain,
...
Mohammed Khazaal Hashim
Published: 31/12/2025
Download PDF
Cite
x
APA
Mezher Hussain, A., Jaber Abed, S. & Khazaal Hashim, M. (2025). Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery, 6(2), 1-6.
MLA
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6.2 (2025): 1-6.
Chicago
Mezher Hussain, Asaad, Sattar Jaber Abed and Mohammed Khazaal Hashim. "Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess." Himalayan Journal of Medicine and Surgery 6, no. 2 (2025): 1-6.
Harvard
Mezher Hussain, A., Jaber Abed, S. and Khazaal Hashim, M. (2025) 'Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess' Himalayan Journal of Medicine and Surgery 6(2), pp. 1-6.
Vancouver
Mezher Hussain A, Jaber Abed S, Khazaal Hashim M. Mean Platelet Volume, Systemic Immune-Inflammation Index and Procalcitonin as Biomarkers in Streptococcal Acute Tonsillitis and Peritonsillar Abscess. Himalayan Journal of Medicine and Surgery. 2025 Jul;6(2):1-6.
Download PDF
Research Article
Amniotic Fluid and Umbilical Cord Serum Erythropoietin as Biomarkers of Fetal Hypoxia in Term and Prolonged Pregnancies
Wasan Salih Mohammed,
Sarah F. Abdulqader
Published: 15/01/2026
Download PDF
Cite
x
APA
Mohammed, W. S. & Abdulqader, S. F. (2026). Amniotic Fluid and Umbilical Cord Serum Erythropoietin as Biomarkers of Fetal Hypoxia in Term and Prolonged Pregnancies. Himalayan Journal of Medicine and Surgery, 7(1), 1-6.
MLA
Mohammed, Wasan Salih and Sarah F. Abdulqader. "Amniotic Fluid and Umbilical Cord Serum Erythropoietin as Biomarkers of Fetal Hypoxia in Term and Prolonged Pregnancies." Himalayan Journal of Medicine and Surgery 7.1 (2026): 1-6.
Chicago
Mohammed, Wasan Salih and Sarah F. Abdulqader. "Amniotic Fluid and Umbilical Cord Serum Erythropoietin as Biomarkers of Fetal Hypoxia in Term and Prolonged Pregnancies." Himalayan Journal of Medicine and Surgery 7, no. 1 (2026): 1-6.
Harvard
Mohammed, W. S. and Abdulqader, S. F. (2026) 'Amniotic Fluid and Umbilical Cord Serum Erythropoietin as Biomarkers of Fetal Hypoxia in Term and Prolonged Pregnancies' Himalayan Journal of Medicine and Surgery 7(1), pp. 1-6.
Vancouver
Mohammed WS, Abdulqader SF. Amniotic Fluid and Umbilical Cord Serum Erythropoietin as Biomarkers of Fetal Hypoxia in Term and Prolonged Pregnancies. Himalayan Journal of Medicine and Surgery. 2026 Jan;7(1):1-6.
Nkole Aboughe, M., Nguema, J. H. N., None, E. C., None, S. I. & Ndong, F. O. (2022). Management of Neonatal Occlusions in the Surgery Department of the Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori in Libreville from January 1, 2019 to December 31, 2021. Himalayan Journal of Medicine and Surgery, 3(2), 1-7.
MLA
Nkole Aboughe, Mélina, et al. "Management of Neonatal Occlusions in the Surgery Department of the Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori in Libreville from January 1, 2019 to December 31, 2021." Himalayan Journal of Medicine and Surgery 3.2 (2022): 1-7.
Chicago
Nkole Aboughe, Mélina, J. H. Nzue Nguema, E. Comlan , S. Ipouka and F. Ondo Ndong. "Management of Neonatal Occlusions in the Surgery Department of the Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori in Libreville from January 1, 2019 to December 31, 2021." Himalayan Journal of Medicine and Surgery 3, no. 2 (2022): 1-7.
Harvard
Nkole Aboughe, M., Nguema, J. H. N., None, E. C., None, S. I. and Ndong, F. O. (2022) 'Management of Neonatal Occlusions in the Surgery Department of the Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori in Libreville from January 1, 2019 to December 31, 2021' Himalayan Journal of Medicine and Surgery 3(2), pp. 1-7.
Vancouver
Nkole Aboughe M, Nguema JHN, E. Comlan EC, S. Ipouka SI, Ndong FO. Management of Neonatal Occlusions in the Surgery Department of the Centre Hospitalier Universitaire Mère-Enfant Fondation Jeanne Ebori in Libreville from January 1, 2019 to December 31, 2021. Himalayan Journal of Medicine and Surgery. 2022 Jul;3(2):1-7.